

Humoral and T-cell responses to SARS-CoV-2 vaccination in patients receiving immunosuppression
- PMID: 34362747
- PMCID: PMC8350975
- DOI: 10.1136/annrheumdis-2021-220626
Humoral and T-cell responses to SARS-CoV-2 vaccination in patients receiving immunosuppression
Abstract
Objective: There is an urgent need to assess the impact of immunosuppressive therapies on the immunogenicity and efficacy of SARS-CoV-2 vaccination.
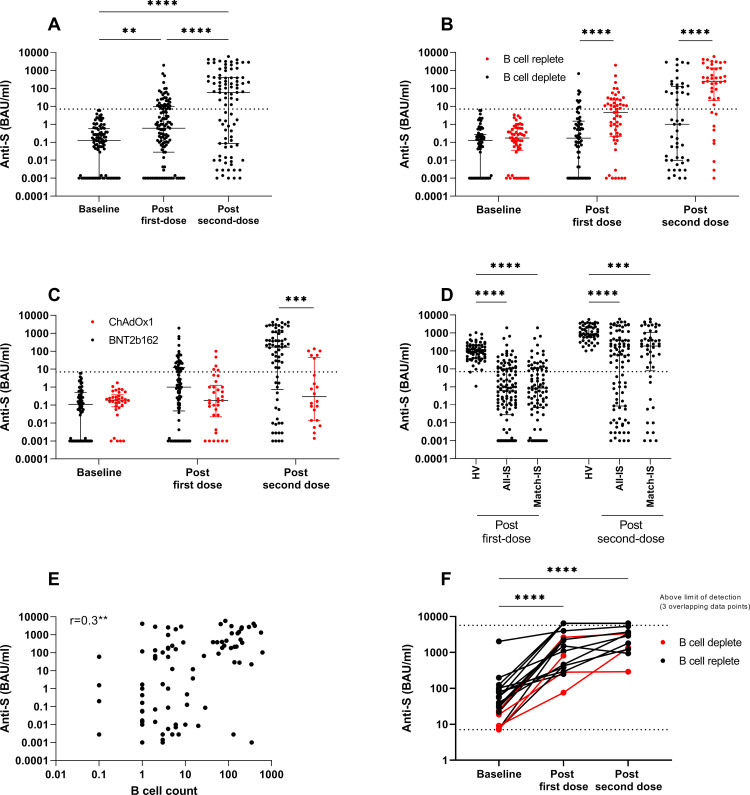
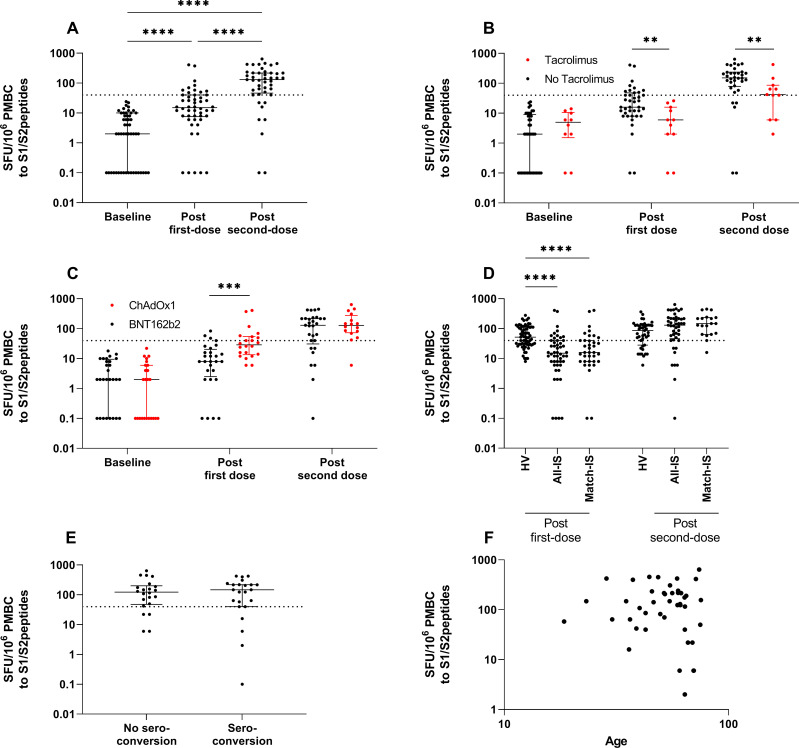
Methods: Serological and T-cell ELISpot assays were used to assess the response to first-dose and second-dose SARS-CoV-2 vaccine (with either BNT162b2 mRNA or ChAdOx1 nCoV-19 vaccines) in 140 participants receiving immunosuppression for autoimmune rheumatic and glomerular diseases.
Results: Following first-dose vaccine, 28.6% (34/119) of infection-naïve participants seroconverted and 26.0% (13/50) had detectable T-cell responses to SARS-CoV-2. Immune responses were augmented by second-dose vaccine, increasing seroconversion and T-cell response rates to 59.3% (54/91) and 82.6% (38/46), respectively. B-cell depletion at the time of vaccination was associated with failure to seroconvert, and tacrolimus therapy was associated with diminished T-cell responses. Reassuringly, only 8.7% of infection-naïve patients had neither antibody nor T-cell responses detected following second-dose vaccine. In patients with evidence of prior SARS-CoV-2 infection (19/140), all mounted high-titre antibody responses after first-dose vaccine, regardless of immunosuppressive therapy.
Conclusion: SARS-CoV-2 vaccines are immunogenic in patients receiving immunosuppression, when assessed by a combination of serology and cell-based assays, although the response is impaired compared with healthy individuals. B-cell depletion following rituximab impairs serological responses, but T-cell responses are preserved in this group. We suggest that repeat vaccine doses for serological non-responders should be investigated as means to induce more robust immunological response.
Keywords: B-lymphocytes; COVID-19; autoimmune diseases; rituximab; vaccination.
© Author(s) (or their employer(s)) 2021. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: PK and MW received support to use the T-SPOT Discovery SARS-CoV-2 by Oxford Immunotec.
Figures
References
-
- UK Department of Health and Social Care; Public Health England . Guidance on shielding and protecting people who are clinically extremely vulnerable from COVID-19, 2021. Available: https://wwwgovuk/government/publications/guidance-on-shielding-and-prote...
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
