

Monogenic Diabetes in Youth With Presumed Type 2 Diabetes: Results From the Progress in Diabetes Genetics in Youth (ProDiGY) Collaboration
- PMID: 34362814
- PMCID: PMC8929184
- DOI: 10.2337/dc21-0491
Monogenic Diabetes in Youth With Presumed Type 2 Diabetes: Results From the Progress in Diabetes Genetics in Youth (ProDiGY) Collaboration
Abstract
Objective: Maturity-onset diabetes of the young (MODY) is frequently misdiagnosed as type 1 or type 2 diabetes. Correct diagnosis may result in a change in clinical treatment and impacts prediction of complications and familial risk. In this study, we aimed to assess the prevalence of MODY in multiethnic youth under age 20 years with a clinical diagnosis of type 2 diabetes.
Research design and methods: We evaluated whole-exome sequence data of youth with a clinical diagnosis of type 2 diabetes. We considered participants to have MODY if they carried a MODY gene variant classified as likely pathogenic (LP) or pathogenic (P) according to current guidelines.
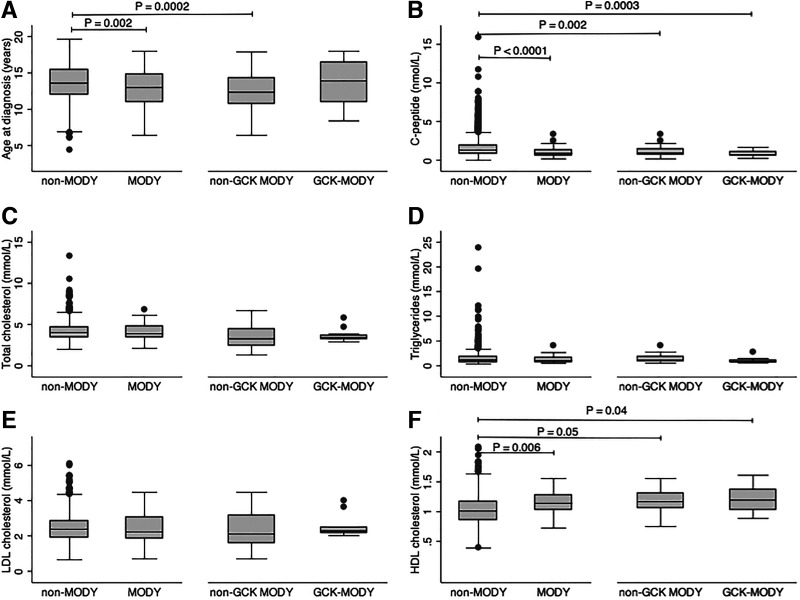
Results: Of 3,333 participants, 93 (2.8%) carried an LP/P variant in HNF4A (16 participants), GCK (23), HNF1A (44), PDX1 (5), INS (4), and CEL (1). Compared with those with no LP/P variants, youth with MODY had a younger age at diagnosis (12.9 ± 2.5 vs. 13.6 ± 2.3 years, P = 0.002) and lower fasting C-peptide levels (3.0 ± 1.7 vs. 4.7 ± 3.5 ng/mL, P < 0.0001). Youth with MODY were less likely to have hypertension (6.9% vs. 19.5%, P = 0.007) and had higher HDL cholesterol (43.8 vs. 39.7 mg/dL, P = 0.006).
Conclusions: By comprehensively sequencing the coding regions of all MODY genes, we identified MODY in 2.8% of youth with clinically diagnosed type 2 diabetes; importantly, in 89% (n = 83) the specific diagnosis would have changed clinical management. No clinical criterion reliably separated the two groups. New tools are needed to find ideal criteria for selection of individuals for genetic testing.
© 2021 by the American Diabetes Association.
Figures
References
-
- Pearson ER, Starkey BJ, Powell RJ, Gribble FM, Clark PM, Hattersley AT. Genetic cause of hyperglycaemia and response to treatment in diabetes. Lancet 2003;362:1275–1281 - PubMed
-
- Pearson ER, Pruhova S, Tack CJ, et al. Molecular genetics and phenotypic characteristics of MODY caused by hepatocyte nuclear factor 4alpha mutations in a large European collection. Diabetologia 2005;48:878–885 - PubMed
-
- Shepherd M, Shields B, Ellard S, Rubio-Cabezas O, Hattersley AT. A genetic diagnosis of HNF1A diabetes alters treatment and improves glycaemic control in the majority of insulin-treated patients. Diabet Med 2009;26:437–441 - PubMed
-
- Hattersley AT, Greeley SAW, Polak M, et al. ISPAD clinical practice consensus guidelines 2018: the diagnosis and management of monogenic diabetes in children and adolescents. Pediatr Diabetes 2018;19(Suppl. 27):47–63 - PubMed
-
- Steele AM, Shields BM, Wensley KJ, Colclough K, Ellard S, Hattersley AT. Prevalence of vascular complications among patients with glucokinase mutations and prolonged, mild hyperglycemia. JAMA 2014;311:279–286 - PubMed
Grants and funding
- P30 DK057516/DK/NIDDK NIH HHS/United States
- UC4 DK108173/DK/NIDDK NIH HHS/United States
- U18 DP006134/DP/NCCDPHP CDC HHS/United States
- M01 RR000069/RR/NCRR NIH HHS/United States
- U01 DP000244/DP/NCCDPHP CDC HHS/United States
- M01 RR014467/RR/NCRR NIH HHS/United States
- U01 DK061230/DK/NIDDK NIH HHS/United States
- U01 DK085526/DK/NIDDK NIH HHS/United States
- U18 DP002708/DP/NCCDPHP CDC HHS/United States
- R01 DK125490/DK/NIDDK NIH HHS/United States
- U01 DK061254/DK/NIDDK NIH HHS/United States
- UL1 RR024139/RR/NCRR NIH HHS/United States
- UL1 RR024989/RR/NCRR NIH HHS/United States
- UL1 RR024153/RR/NCRR NIH HHS/United States
- U18 DP006131/DP/NCCDPHP CDC HHS/United States
- U01 DP000247/DP/NCCDPHP CDC HHS/United States
- U54 HG003067/HG/NHGRI NIH HHS/United States
- U18 DP002710/DP/NCCDPHP CDC HHS/United States
- K23 DK120932/DK/NIDDK NIH HHS/United States
- U18 DP006138/DP/NCCDPHP CDC HHS/United States
- UL1 RR025780/RR/NCRR NIH HHS/United States
- UL1 TR000154/TR/NCATS NIH HHS/United States
- M01 RR000036/RR/NCRR NIH HHS/United States
- U18 DP002714/DP/NCCDPHP CDC HHS/United States
- U01 DK061242/DK/NIDDK NIH HHS/United States
- K12 DK094721/DK/NIDDK NIH HHS/United States
- U01 DP000248/DP/NCCDPHP CDC HHS/United States
- UL1 RR024992/RR/NCRR NIH HHS/United States
- UL1 TR000062/TR/NCATS NIH HHS/United States
- U01 DK061212/DK/NIDDK NIH HHS/United States
- M01 RR001066/RR/NCRR NIH HHS/United States
- T32 DK007161/DK/NIDDK NIH HHS/United States
- P30 DK098722/DK/NIDDK NIH HHS/United States
- U18 DP006136/DP/NCCDPHP CDC HHS/United States
- U18 DP002709/DP/NCCDPHP CDC HHS/United States
- U18 DP006133/DP/NCCDPHP CDC HHS/United States
- M01 RR000043/RR/NCRR NIH HHS/United States
- UL1 TR001425/TR/NCATS NIH HHS/United States
- U18 DP006139/DP/NCCDPHP CDC HHS/United States
- UL1 RR025758/RR/NCRR NIH HHS/United States
- UL1 TR000077/TR/NCATS NIH HHS/United States
- R01 DK127208/DK/NIDDK NIH HHS/United States
- UL1 TR000423/TR/NCATS NIH HHS/United States
- M01 RR000084/RR/NCRR NIH HHS/United States
- U01 DP000250/DP/NCCDPHP CDC HHS/United States
- K24 HL157960/HL/NHLBI NIH HHS/United States
- U01 DP000246/DP/NCCDPHP CDC HHS/United States
- U01 DP000254/DP/NCCDPHP CDC HHS/United States
- M01 RR000125/RR/NCRR NIH HHS/United States
- U01 DK061239/DK/NIDDK NIH HHS/United States
- UL1 RR024134/RR/NCRR NIH HHS/United States
LinkOut - more resources
Full Text Sources
Miscellaneous
