

Cerebrospinal fluid flow cytometry distinguishes psychosis spectrum disorders from differential diagnoses
- PMID: 34363013
- PMCID: PMC8873003
- DOI: 10.1038/s41380-021-01244-5
Cerebrospinal fluid flow cytometry distinguishes psychosis spectrum disorders from differential diagnoses
Abstract
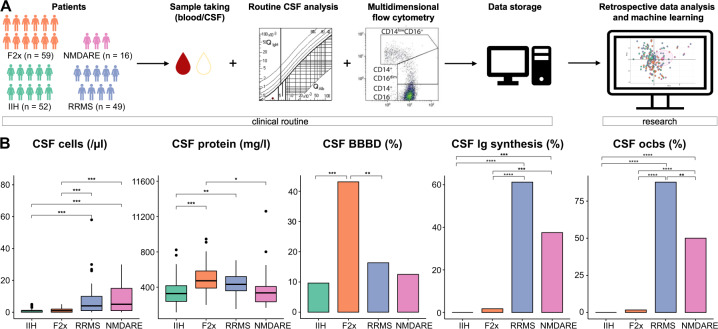
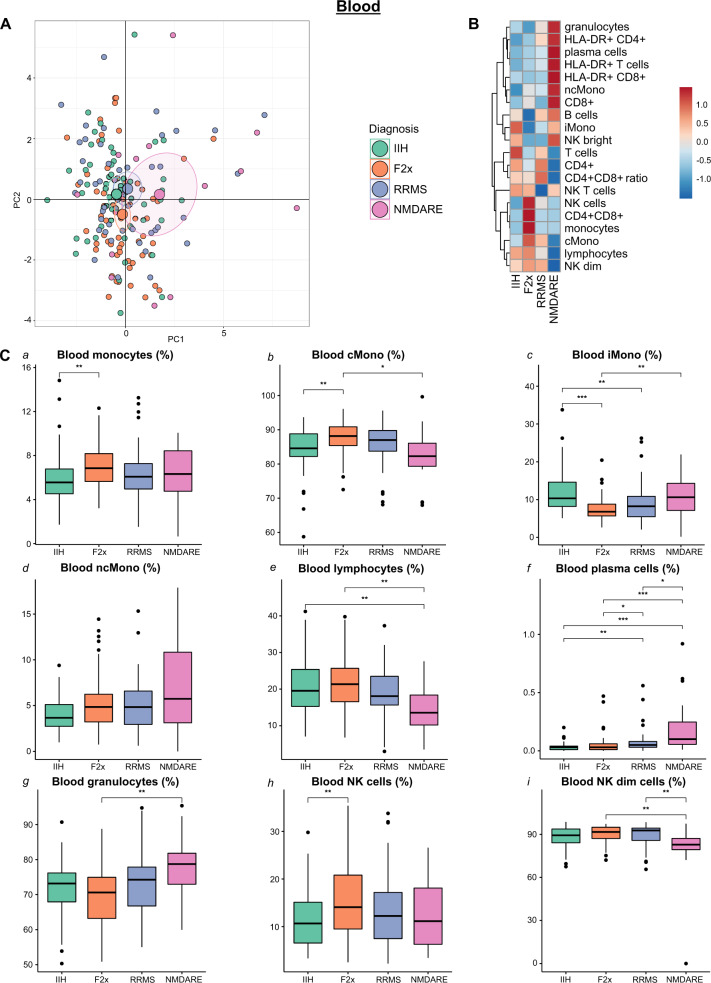
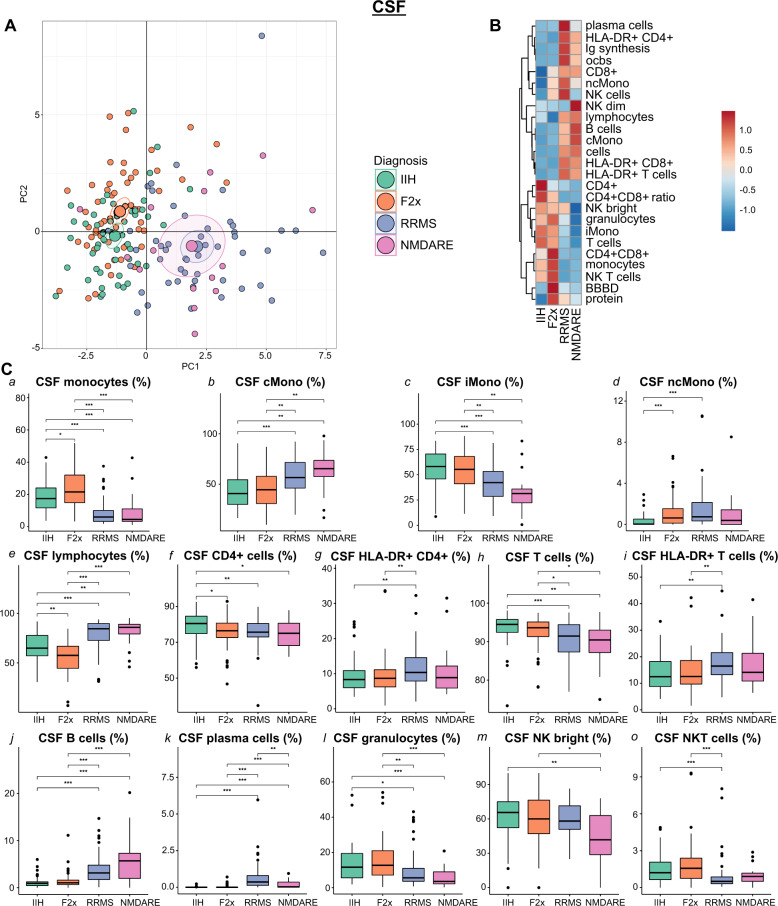
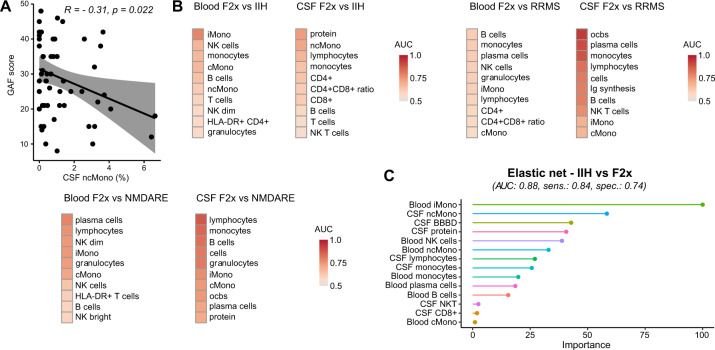
Psychotic disorders are common and disabling mental conditions. The relative importance of immune-related mechanisms in psychotic disorders remains subject of debate. Here, we present a large-scale retrospective study of blood and cerebrospinal fluid (CSF) immune cell profiles of psychosis spectrum patients. We performed basic CSF analysis and multi-dimensional flow cytometry of CSF and blood cells from 59 patients with primary psychotic disorders (F20, F22, F23, and F25) in comparison to inflammatory (49 RRMS and 16 NMDARE patients) and non-inflammatory controls (52 IIH patients). We replicated the known expansion of monocytes in the blood of psychosis spectrum patients, that we identified to preferentially affect classical monocytes. In the CSF, we found a relative shift from lymphocytes to monocytes, increased protein levels, and evidence of blood-brain barrier disruption in psychosis. In fact, these CSF features confidently distinguished autoimmune encephalitis from psychosis despite similar (initial) clinical features. We then constructed machine learning models incorporating blood and CSF parameters and demonstrated their superior ability to differentiate psychosis from non-inflammatory controls compared to individual parameters. Multi-dimensional and multi-compartment immune cell signatures can thus support the diagnosis of psychosis spectrum disorders with the potential to accelerate diagnosis and initiation of therapy.
© 2021. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- National Collaborating Centre for Mental Health (UK . Psychosis and schizophrenia in adults: treatment and management: updated edition 2014. London: National Institute for Health and Care Excellence (UK); 2014. - PubMed
-
- Carpenter WT, Strauss JS, Bartko JJ. The diagnosis and understanding of schizophrenia. Part I. Use of signs and symptoms for the identification of schizophrenic patients. Schizophr Bull. 1974;11:37–49. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
