

18F-FDG PET/CT in Infective Endocarditis: Indications and Approaches for Standardization
- PMID: 34363148
- PMCID: PMC8346431
- DOI: 10.1007/s11886-021-01542-y
18F-FDG PET/CT in Infective Endocarditis: Indications and Approaches for Standardization
Abstract
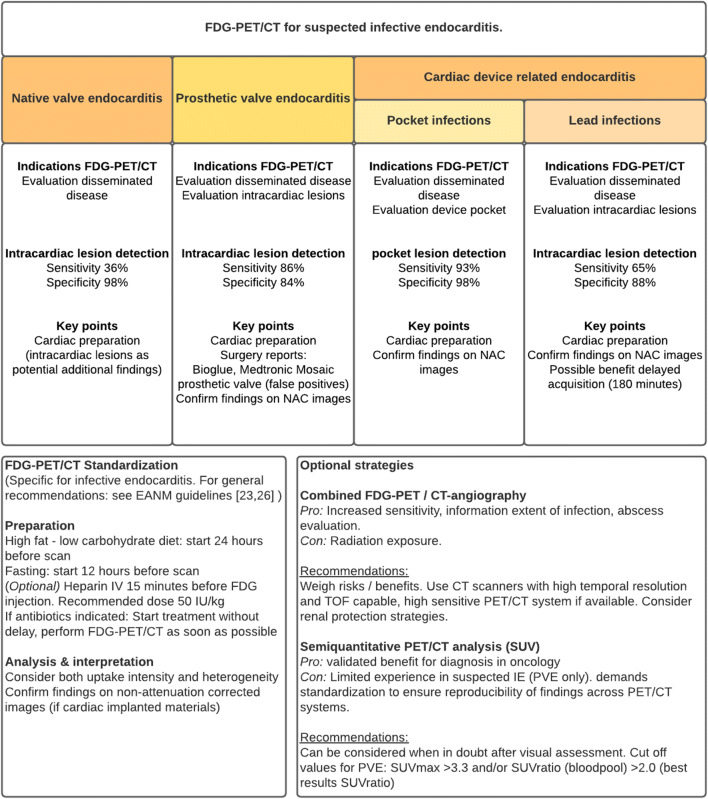
Purpose of review: Additional imaging modalities, such as FDG-PET/CT, have been included into the workup for patients with suspected infective endocarditis, according to major international guidelines published in 2015. The purpose of this review is to give an overview of FDG-PET/CT indications and standardized approaches in the setting of suspected infective endocarditis.
Recent findings: There are two main indications for performing FDG-PET/CT in patients with suspected infective endocarditis: (i) detecting intracardiac infections and (ii) detection of (clinically silent) disseminated infectious disease. The diagnostic performance of FDG-PET/CT for intracardiac lesions depends on the presence of native valves, prosthetic valves, or implanted cardiac devices, with a sensitivity that is poor for native valve endocarditis and cardiac device-related lead infections, but much better for prosthetic valve endocarditis and cardiac device-related pocket infections. Specificity is high for all these indications. The detection of disseminated disease may also help establish the diagnosis and/or impact patient management. Based on current evidence, FDG-PET/CT should be considered for detection of disseminated disease in suspected endocarditis. Absence of intracardiac lesions on FDG-PET/CT cannot rule out native valve endocarditis, but positive findings strongly support the diagnosis. For prosthetic valve endocarditis, standard use of FDG-PET/CT is recommended because of its high sensitivity and specificity. For implanted cardiac devices, FDG-PET/CT is also recommended, but should be evaluated with careful attention to clinical context, because its sensitivity is high for pocket infections, but low for lead infections. In patients with prosthetic valves with or without additional aortic prosthesis, combination with CTA should be considered. Optimal timing of FDG-PET/CT is important, both during clinical workup and technically (i.e., post tracer injection). In addition, procedural standardization is key and encompasses patient preparation, scan acquisition, reconstruction, subsequent analysis, and clinical interpretation. The recommendations discussed here will hopefully contribute to improved standardization and enhanced performance of FDG-PET/CT in the clinical management of patients with suspected infective endocarditis.
Keywords: Endocarditis; FDG; Indications; PET/CT; Standardization.
© 2021. The Author(s).
Conflict of interest statement
Dr. ten Hove, Dr. Glaudemans, Dr. Slart, and Dr. Sinha report the aforementioned institutional funding through PUSH. Additionally, Dr. Sinha reports grants from Beatrixoord Foundation, grants from the European Union, outside the submitted work, and Committee work (executive boards) on a local and national level dealing with guideline development of infections. Dr. Budde reports grants from HeartFlow and Siemens, outside the submitted work.
Figures
References
-
- Jensen AD, Bundgaard H, Butt JH, Bruun NE, Voldstedlund M, Torp-Pedersen C, Gislason G, Iversen K, Chamat S, Dahl A, Køber L, Østergaard L, Fosbøl EL. Temporal changes in the incidence of infective endocarditis in Denmark 1997-2017: a nationwide study. Int J Cardiol. 2021;326:145–152. doi: 10.1016/j.ijcard.2020.10.029. - DOI - PubMed
-
- Heredia-Rodríguez M, Hernández A, Bustamante-Munguira J, Álvarez FJ, Eiros JM, Castrodeza J, Tamayo E. Evolution of the incidence, mortality, and cost of infective endocarditis in Spain between 1997 and 2014. J Gen Intern Med. 2018;33(10):1610–1613. doi: 10.1007/s11606-018-4514-7. - DOI - PMC - PubMed
-
- van den Brink FS, Swaans MJ, Hoogendijk MG, Alipour A, Kelder JC, Jaarsma W, Eefting FD, Groenmeijer B, Kupper AJF, Ten Berg JM. Increased incidence of infective endocarditis after the 2009 European Society of Cardiology guideline update: a nationwide study in the Netherlands. Eur Heart J Qual Care Clin Outcomes. 2017;3(2):141–147. - PubMed
-
- Sunder S, Grammatico-Guillon L, Lemaignen A, Lacasse M, Gaborit C, Boutoille D, Tattevin P, Denes E, Guimard T, Dupont M, Fauchier L, Bernard L. Incidence, characteristics, and mortality of infective endocarditis in France in 2011. PLoS One. 2019;14(10):e0223857. doi: 10.1371/journal.pone.0223857. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
