

Coronary Artery Anomalies and Their Impact on the Feasibility of Percutaneous Pulmonary Valve Implantation
- PMID: 34363499
- PMCID: PMC8766387
- DOI: 10.1007/s00246-021-02684-0
Coronary Artery Anomalies and Their Impact on the Feasibility of Percutaneous Pulmonary Valve Implantation
Abstract
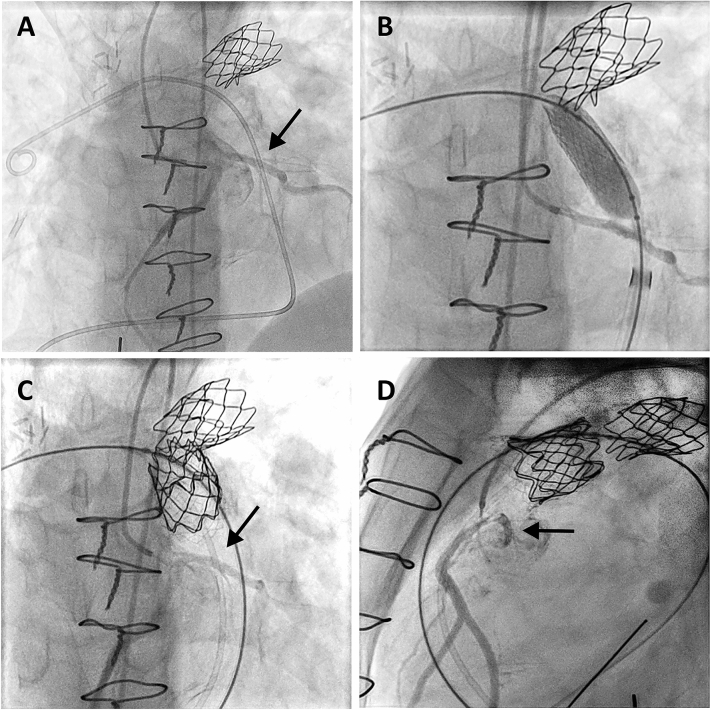
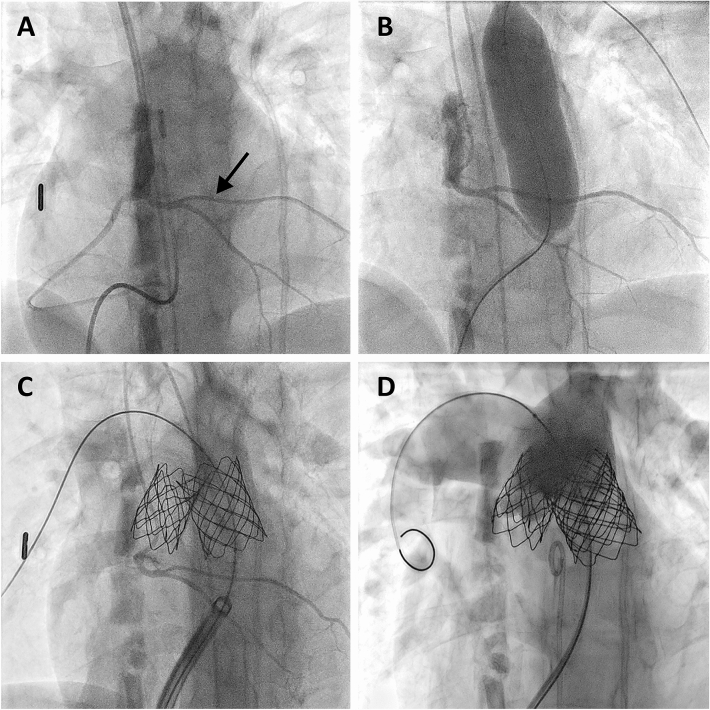
One of the major obstacles preventing successful percutaneous pulmonary valve implantation (PPVI) is related to the close proximity of coronary artery branches to the expected landing zone. The aim of this study was to assess the frequency of coronary artery anomalies (CAAs) especially those associated with major coronary branches crossing the right ventricular outflow tract (RVOT) and to describe their relevance for the feasibility of percutaneous pulmonary valve implantation (PPVI). In our retrospective single-center study 90 patients were evaluated who underwent invasive testing for PPVI in our institution from 1/2010 to 1/2020. CAAs were identified in seven patients (8%) associated with major branches crossing the RVOT due to origin of the left anterior descending (LAD) or a single coronary artery from the right aortic sinus. In 5/7 patients with CAAs balloon testing of the RVOT and selective coronary angiographies revealed a sufficiently large landing zone distal to the coronary artery branch. While unfavorable RVOT dimensions prevented PPVI in one, PPVI was performed successfully in the remaining four patients. The relatively short landing zone required application of the "folded" melody technique in two patients. All patients are doing well (mean follow-up 3 years). CAAs associated with major coronary branches crossing the RVOT can be expected in about 8% of patients who are potential candidates for PPVI. Since the LAD crossed the RVOT below the plane of the pulmonary valve successful distal implantation of the valve was possible in 4/7 patients. Therefore these coronary anomalies should not be considered as primary contraindications for PPVI.
Keywords: Congenital coronary artery anomaly; Congenital heart disease; Percutaneous pulmonary valve implantation.
© 2021. The Author(s).
Conflict of interest statement
A. Hanser and A. Hornung have received research grants from the “Stiftung zur Förderung der Erforschung der Zivilisationerkrankungen.” A. Hanser reports grants from the Deutsche Herzstiftung e.V. The other authors have no relevant financial or non-financial interests to disclose.
Figures
References
-
- Cabalka AK, Hellenbrand WE, Eicken A, Kreutzer J, Gray RG, Bergersen L, Berger F, Armstrong AK, Cheatham JP, Zahn EM, McElhinney DB. Relationships among conduit type, pre-stenting, and outcomes in patients undergoing transcatheter pulmonary valve replacement in the prospective North American and European melody valve trials. JACC Cardiovasc Interv. 2017;10:1746–1759. doi: 10.1016/j.jcin.2017.05.022. - DOI - PubMed
-
- Cheatham JP, Hellenbrand WE, Zahn EM, Jones TK, Berman DP, Vincent JA, McElhinney DB. Clinical and hemodynamic outcomes up to 7 years after transcatheter pulmonary valve replacement in the US melody valve investigational device exemption trial. Circulation. 2015;131:1960–1970. doi: 10.1161/CIRCULATIONAHA.114.013588. - DOI - PubMed
-
- Nordmeyer J, Ewert P, Gewillig M, AlJufan M, Carminati M, Kretschmar O, Uebing A, Dahnert I, Rohle R, Schneider H, Witsenburg M, Benson L, Gitter R, Bokenkamp R, Mahadevan V, Berger F. Acute and midterm outcomes of the post-approval MELODY Registry: a multicentre registry of transcatheter pulmonary valve implantation. Eur Heart J. 2019;40:2255–2264. doi: 10.1093/eurheartj/ehz201. - DOI - PubMed
-
- Fraisse A, Assaidi A, Mauri L, Malekzadeh-Milani S, Thambo JB, Bonnet D, Iserin L, Mancini J, Boudjemline Y. Coronary artery compression during intention to treat right ventricle outflow with percutaneous pulmonary valve implantation: incidence, diagnosis, and outcome. Catheter Cardiovasc Interv. 2014;83:E260–268. doi: 10.1002/ccd.25471. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
