

Thromboembolism risk among patients with diabetes/stress hyperglycemia and COVID-19
- PMID: 34364927
- PMCID: PMC8340557
- DOI: 10.1016/j.metabol.2021.154845
Thromboembolism risk among patients with diabetes/stress hyperglycemia and COVID-19
Abstract
Purpose: Individuals with diabetes/stress hyperglycemia carry an increased risk for adverse clinical outcome in case of SARS-CoV-2 infection. The purpose of this study was to evaluate whether this risk is, at least in part, modulated by an increase of thromboembolic complications.
Methods: We prospectively followed 180 hospitalized patients with confirmed COVID-19 pneumonia admitted to the Internal Medicine Units of San Raffaele Hospital. Data from 11 out of 180 patients were considered incomplete and excluded from the analysis. We analysed inflammation, tissue damage biomarkers, hemostatic parameters, thrombotic events (TEs) and clinical outcome according to the presence of diabetes/stress hyperglycemia.
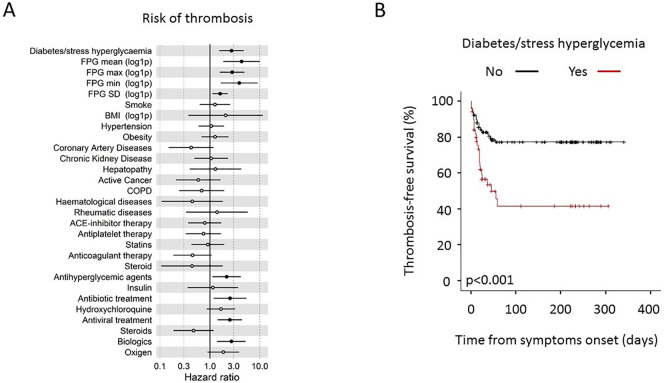
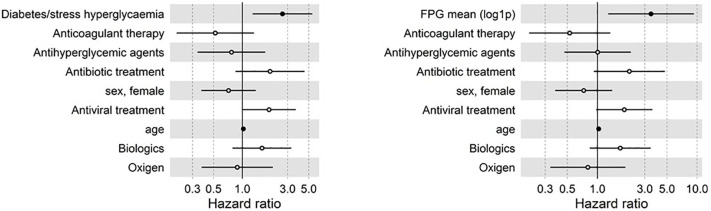
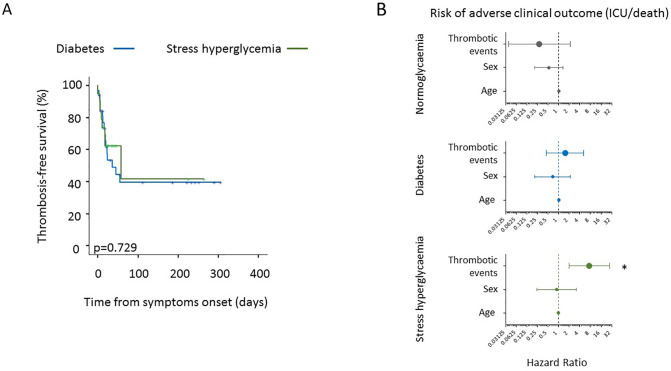
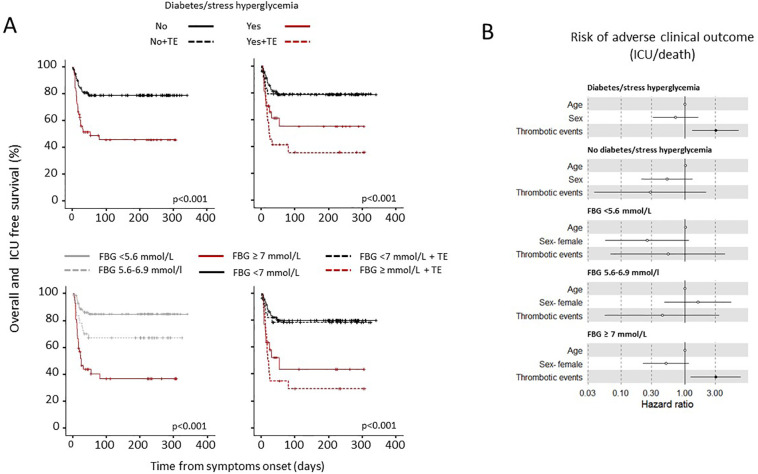
Results: Among 169 patients, 51 (30.2%) had diabetes/stress hyperglycemia. Diabetes/stress hyperglycemia and fasting blood glucose (FBG) were associated with increased inflammation and tissue damage circulating markers, higher D-dimer levels, increased prothrombin time and lower antithrombin III activity. Forty-eight venous and 10 arterial TEs were identified in 49 (29%) patients. Diabetes/stress hyperglycemia (HR 2.71, p = 0.001), fasting blood glucose (HR 4.32, p < 0.001) and glucose variability (HR 1.6, p < 0.009) were all associated with an increased risk of thromboembolic complication. TEs significantly increased the risk for an adverse clinical outcome only in the presence of diabetes/stress hyperglycemia (HR 3.05, p = 0.010) or fasting blood glucose ≥7 mmol/L (HR 3.07, p = 0.015).
Conclusions: Thromboembolism risk is higher among patients with diabetes/stress hyperglycemia and COVID-19 pneumonia and is associated to poor clinical outcome. In case of SARS-Cov-2 infection patients with diabetes/stress hyperglycemia could be considered for a more intensive prophylactic anticoagulation regimen.
Keywords: COVID-19; Clinical outcome; Diabetes; Humoral response; SARS-CoV-2; Thromboembolism.
Copyright © 2021 Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of competing interest The authors have no conflict of interest to disclose in relation to the topic of this manuscript. The authors declare that there are no relationships or activities that might bias, or be perceived to bias, their work. This work was funded by Program Project COVID-19 OSR-UniSR and COVID-2020-12371617Ministero della Salute.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
