

Methamphetamine-Associated Heart Failure Hospitalizations Across the United States: Geographic and Social Disparities
- PMID: 34365802
- PMCID: PMC8475042
- DOI: 10.1161/JAHA.120.018370
Methamphetamine-Associated Heart Failure Hospitalizations Across the United States: Geographic and Social Disparities
Abstract
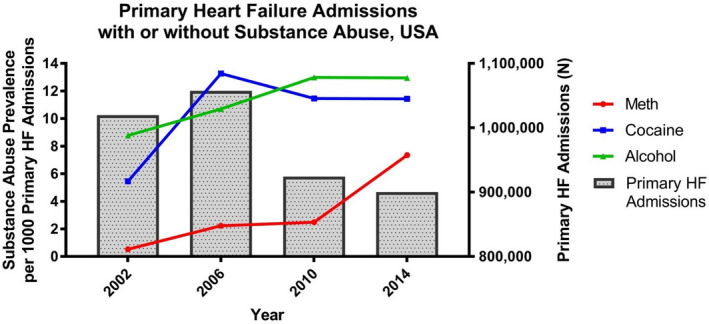
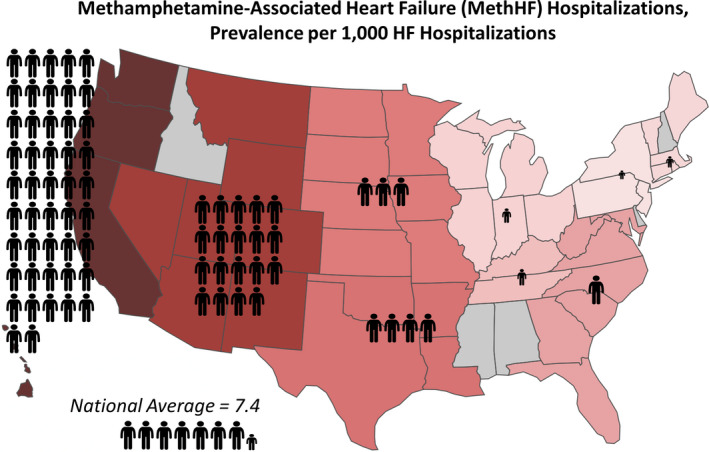
Background Although methamphetamine abuse is associated with the development of heart failure (HF), nationwide data on methamphetamine-associated HF (MethHF) hospitalizations are limited. This study evaluates nationwide HF hospitalizations associated with substance abuse to better understand MethHF prevalence trends and the clinical characteristics of those patients. Methods and Results This cross-sectional period-prevalence study used hospital discharge data from the National Inpatient Sample to identify adult primary HF hospitalizations with a secondary diagnosis of abuse of methamphetamines, cocaine, or alcohol in the United States from 2002 to 2014. All 2014 MethHF admissions were separated by regional census division to evaluate geographical distribution. Demographics, payer information, and clinical characteristics of MethHF hospitalizations were compared with all other HF hospitalizations. Total nationwide MethHF hospitalizations increased from 547 in 2002 to 6625 in 2014 with a predominance on the West Coast. Methamphetamine abuse was slightly more common among primary HF hospitalizations compared with all-cause hospitalizations (7.4 versus 6.4 per 1000; Cohen h=0.012; P<0.001). Among HF hospitalizations, patients with MethHF were younger (mean age, 48.9 versus 72.4 years; Cohen d=1.93; P<0.001), more likely to be on Medicaid (59.4% versus 8.8%; Cohen h=1.16; P<0.001) or uninsured (12.0% versus 2.6%; Cohen h=0.36; P<0.001), and more likely to present to urban hospitals (43.8% versus 28.3%; Cohen h=0.32; P<0.001) than patients with non-methamphetamine associated HF. Patients with MethHF had higher rates of psychiatric comorbidities and were more likely to leave the hospital against medical advice. Conclusions MethHF hospitalizations have significantly increased in the United States, particularly on the West Coast. Coordinated public health policies and systems of care are needed to address this rising epidemic.
Keywords: alcohol; cardiac hospitalization; cardiotoxicity; cocaine; heart failure.
Conflict of interest statement
None.
Figures
References
-
- Diercks DB, Fonarow GC, Kirk JD, Jois‐Bilowich P, Hollander JE, Weber JE, Wynne J, Mills RM, Yancy C, Peacock WF IVth, et al. Illicit stimulant use in a United States heart failure population presenting to the emergency department (from the Acute Decompensated Heart Failure National Registry Emergency Module). Am J Cardiol. 2008;102:1216–1219. DOI: 10.1016/j.amjcard.2008.06.045. - DOI - PubMed
-
- Schürer S, Klingel K, Sandri M, Majunke N, Besler C, Kandolf R, Lurz P, Luck M, Hertel P, Schuler G, et al. Clinical characteristics, histopathological features, and clinical outcome of methamphetamine‐associated cardiomyopathy. JACC Heart Fail. 2017;5:435–445. DOI: 10.1016/j.jchf.2017.02.017. - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
