

One-year follow-up of chest CT findings in patients after SARS-CoV-2 infection
- PMID: 34365975
- PMCID: PMC8349604
- DOI: 10.1186/s12916-021-02056-8
One-year follow-up of chest CT findings in patients after SARS-CoV-2 infection
Abstract
Background: Knowledge about the 1-year outcome of COVID-19 is limited. The aim of this study was to follow-up and evaluate lung abnormalities on serial computed tomography (CT) scans in patients with COVID-19 after hospital discharge.
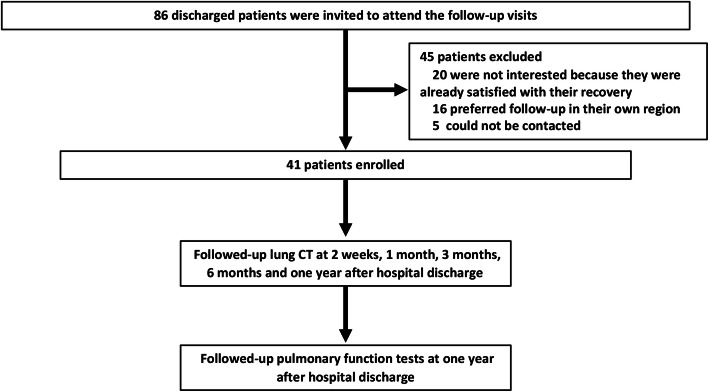
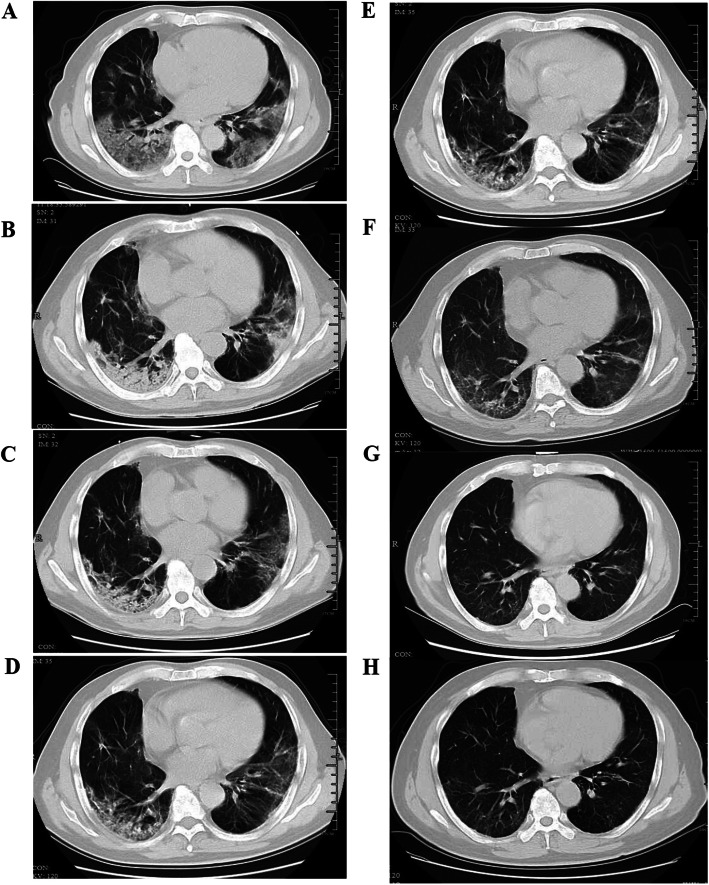
Methods: A prospective cohort study of patients with COVID-19 from the First Affiliated Hospital, Zhejiang University School of Medicine was conducted, with assessments of chest CT during hospitalization and at 2 weeks, 1 month, 3 months, 6 months, and 1 year after hospital discharge. Risk factors of residual CT opacities and the influence of residual CT abnormalities on pulmonary functions at 1 year were also evaluated.
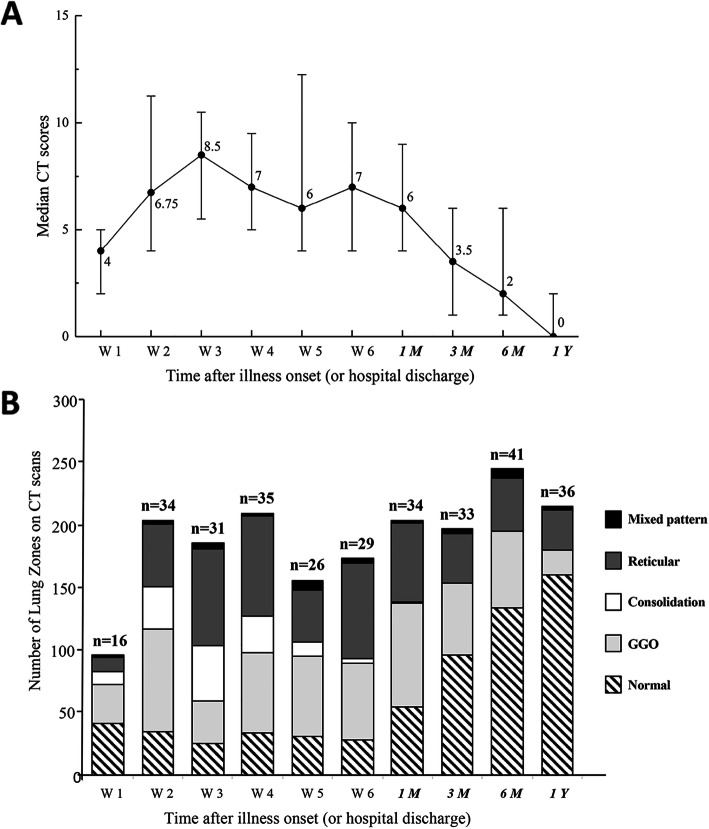
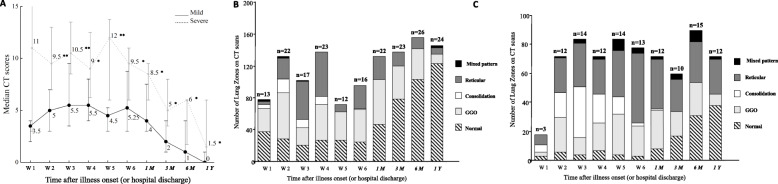
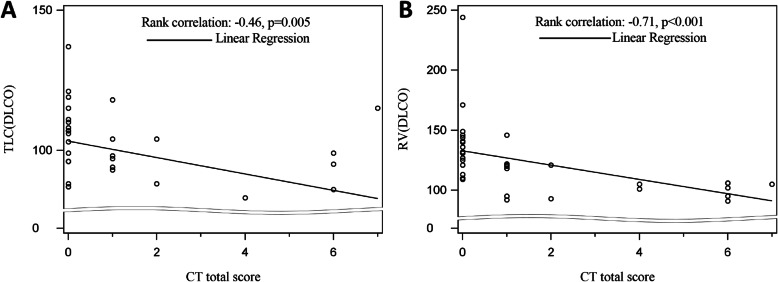
Results: A total of 41 patients were followed in this study. Gradual recovery after hospital discharge was confirmed by the serial CT scores. Around 47% of the patients showed residual aberration on pulmonary CT with a median CT score of 0 (interquartile range (IQR) of 0-2) at 1 year after discharge, with ground-glass opacity (GGO) with reticular pattern as the major radiologic pattern. Patients with residual radiological abnormalities were older (p = 0.01), with higher rate in current smokers (p = 0.04), higher rate in hypertensives (p = 0.05), lower SaO2 (p = 0.004), and higher prevalence of secondary bacterial infections during acute phase (p = 0.02). Multiple logistic regression analyses indicated that age was a risk factor associated with residual radiological abnormalities (OR 1.08, 95% CI 1.01-1.15, p = 0.02). Pulmonary functions of total lung capacity (p = 0.008) and residual volume (p < 0.001) were reduced in patients with residual CT abnormalities and were negatively correlated with CT scores.
Conclusion: During 1-year follow-up after discharge, COVID-19 survivors showed continuous improvement on chest CT. However, residual lesions could still be observed and correlated with lung volume parameters. The risk of developing residual CT opacities increases with age.
Keywords: Convalescence; Lung function; Pulmonary radiography; Risk factors; SARS-CoV-2; Yanfei Chen, Cheng Ding, and Ling Yu contributed equally to the manuscript..
© 2021. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- WHO Coronavirus Disease (COVID-19) Dashboard. https://covid19.who.int. Accessed 1 Nov 2020.
-
- Hui DS, Joynt GM, Wong KT, Gomersall CD, Li TS, Antonio G, Ko FW, Chan MC, Chan DP, Tong MW, Rainer TH, Ahuja AT, Cockram CS, Sung JJ. Impact of severe acute respiratory syndrome (SARS) on pulmonary function, functional capacity and quality of life in a cohort of survivors. Thorax. 2005;60(5):401–409. doi: 10.1136/thx.2004.030205. - DOI - PMC - PubMed
-
- Park WB, Jun KI, Kim G, Choi J-P, Rhee J-Y, Cheon S, Lee CH, Park JS, Kim Y, Joh JS, Chin BS, Choe PG, Bang JH, Park SW, Kim NJ, Lim DG, Kim YS, Oh MD, Shin HS. Correlation between pneumonia severity and pulmonary complications in Middle East respiratory syndrome. J Korean Med Sci. 2018;33(24):e169. doi: 10.3346/jkms.2018.33.e169. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
