

A Framework for Sensor-Based Assessment of Upper-Limb Functioning in Hemiparesis
- PMID: 34366809
- PMCID: PMC8341809
- DOI: 10.3389/fnhum.2021.667509
A Framework for Sensor-Based Assessment of Upper-Limb Functioning in Hemiparesis
Abstract
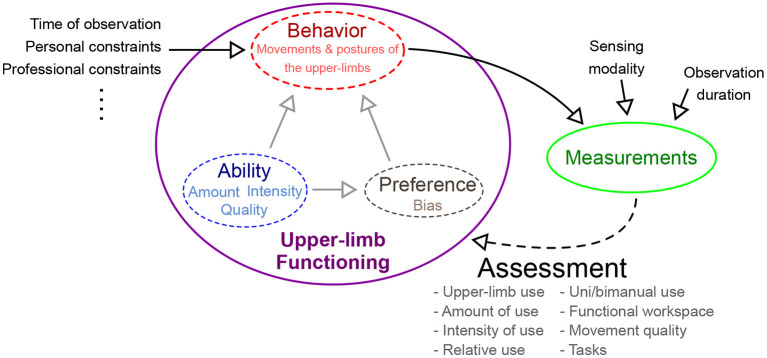
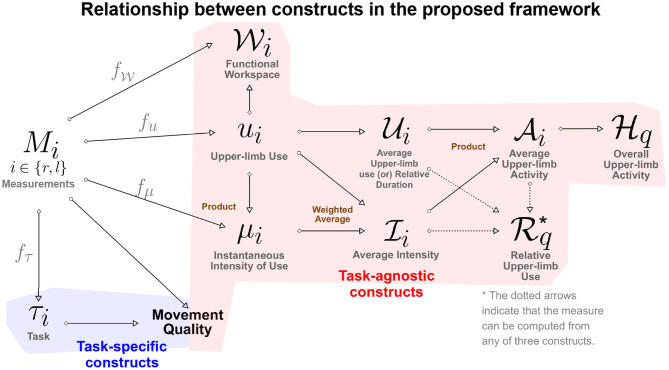
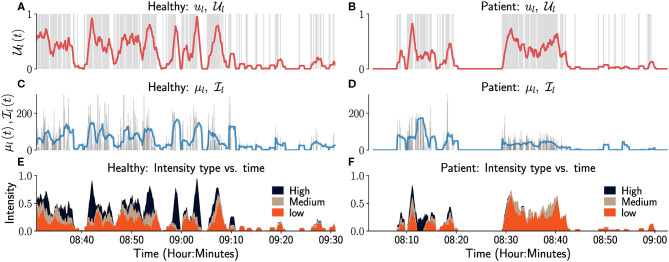
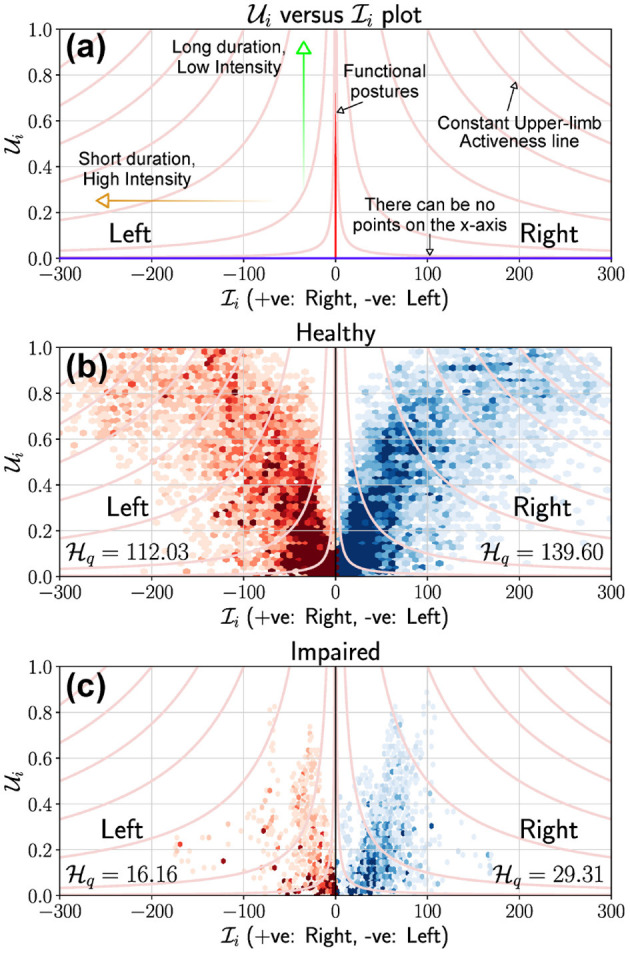
The ultimate goal of any upper-limb neurorehabilitation procedure is to improve upper-limb functioning in daily life. While clinic-based assessments provide an assessment of what a patient can do, they do not completely reflect what a patient does in his/her daily life. The use of compensatory strategies such as the use of the less affected upper-limb or excessive use of trunk in daily life is a common behavioral pattern seen in patients with hemiparesis. To this end, there has been an increasing interest in the use of wearable sensors to objectively assess upper-limb functioning. This paper presents a framework for assessing upper-limb functioning using sensors by providing: (a) a set of definitions of important constructs associated with upper-limb functioning; (b) different visualization methods for evaluating upper-limb functioning; and (c) two new measures for quantifying how much an upper-limb is used and the relative bias in their use. The demonstration of some of these components is presented using data collected from inertial measurement units from a previous study. The proposed framework can help guide the future technical and clinical work in this area to realize valid, objective, and robust tools for assessing upper-limb functioning. This will in turn drive the refinement and standardization of the assessment of upper-limb functioning.
Keywords: arm and hand use; framework; hemiparesis; real world activity; sensorimotor assessment; stroke rehabilitation; upper-limb rehabilitation; wearable sensors.
Copyright © 2021 David, Subash, Varadhan, Melendez-Calderon and Balasubramanian.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
LinkOut - more resources
Full Text Sources