

Sensorimotor Integration in Childhood Dystonia and Dystonic Cerebral Palsy-A Developmental Perspective
- PMID: 34367047
- PMCID: PMC8343097
- DOI: 10.3389/fneur.2021.668081
Sensorimotor Integration in Childhood Dystonia and Dystonic Cerebral Palsy-A Developmental Perspective
Abstract
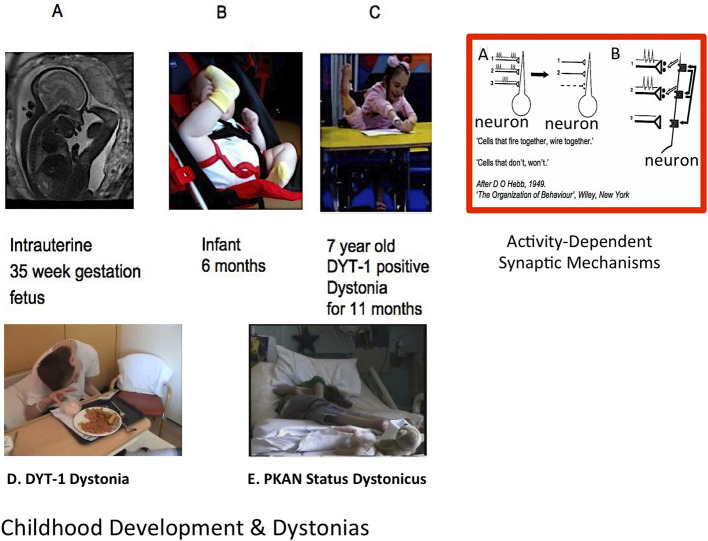
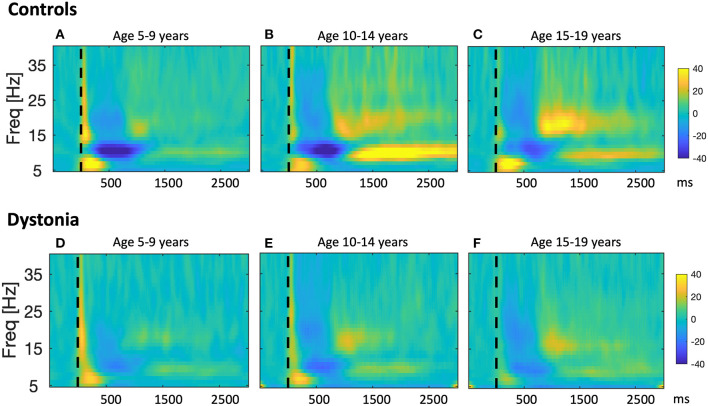
Dystonia is a disorder of sensorimotor integration, involving dysfunction within the basal ganglia, cortex, cerebellum, or their inter-connections as part of the sensorimotor network. Some forms of dystonia are also characterized by maladaptive or exaggerated plasticity. Development of the neuronal processes underlying sensorimotor integration is incompletely understood but involves activity-dependent modeling and refining of sensorimotor circuits through processes that are already taking place in utero and which continue through infancy, childhood, and into adolescence. Several genetic dystonias have clinical onset in early childhood, but there is evidence that sensorimotor circuit development may already be disrupted prenatally in these conditions. Dystonic cerebral palsy (DCP) is a form of acquired dystonia with perinatal onset during a period of rapid neurodevelopment and activity-dependent refinement of sensorimotor networks. However, physiological studies of children with dystonia are sparse. This discussion paper addresses the role of neuroplasticity in the development of sensorimotor integration with particular focus on the relevance of these mechanisms for understanding childhood dystonia, DCP, and implications for therapy selection, including neuromodulation and timing of intervention.
Keywords: children; critical windows; dystonia; dystonic cerebral palsy; neurodevelopment; neuromodulation; plasticity; sensorimotor integration.
Copyright © 2021 McClelland and Lin.
Conflict of interest statement
J-PL received unrestricted educational support for instructional courses and consultancy fees from Medtronic Ltd. The remaining author declares that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures

Similar articles
-
Function and dysfunction of the dystonia network: an exploration of neural circuits that underlie the acquired and isolated dystonias.Dystonia. 2023;2:11805. doi: 10.3389/dyst.2023.11805. Epub 2023 Dec 13. Dystonia. 2023. PMID: 38273865 Free PMC article.
-
EEG measures of sensorimotor processing and their development are abnormal in children with isolated dystonia and dystonic cerebral palsy.Neuroimage Clin. 2021;30:102569. doi: 10.1016/j.nicl.2021.102569. Epub 2021 Jan 19. Neuroimage Clin. 2021. PMID: 33583764 Free PMC article.
-
Dystonia in Childhood: How Insights from Paediatric Research Enrich the Network Theory of Dystonia.Adv Neurobiol. 2023;31:1-22. doi: 10.1007/978-3-031-26220-3_1. Adv Neurobiol. 2023. PMID: 37338693
-
Neuroplasticity in dystonia: Motor symptoms and beyond.Handb Clin Neurol. 2022;184:207-218. doi: 10.1016/B978-0-12-819410-2.00031-X. Handb Clin Neurol. 2022. PMID: 35034735 Review.
-
Contemporary functional neuroanatomy and pathophysiology of dystonia.J Neural Transm (Vienna). 2021 Apr;128(4):499-508. doi: 10.1007/s00702-021-02299-y. Epub 2021 Jan 24. J Neural Transm (Vienna). 2021. PMID: 33486625 Free PMC article. Review.
Cited by
-
Function and dysfunction of the dystonia network: an exploration of neural circuits that underlie the acquired and isolated dystonias.Dystonia. 2023;2:11805. doi: 10.3389/dyst.2023.11805. Epub 2023 Dec 13. Dystonia. 2023. PMID: 38273865 Free PMC article.
-
EEG-based sensorimotor neurofeedback for motor neurorehabilitation in children and adults: A scoping review.Clin Neurophysiol. 2024 Nov;167:143-166. doi: 10.1016/j.clinph.2024.08.009. Epub 2024 Aug 20. Clin Neurophysiol. 2024. PMID: 39321571 Free PMC article.
-
Cortical Oscillatory Activity and Motor Control in Pediatric Stroke Patients With Hemidystonia.Hum Brain Mapp. 2025 Apr 1;46(5):e70204. doi: 10.1002/hbm.70204. Hum Brain Mapp. 2025. PMID: 40186512 Free PMC article.
-
Bibliometric analysis of hot literature on neural circuit research.Ibrain. 2023 Dec 21;10(1):69-82. doi: 10.1002/ibra.12144. eCollection 2024 Spring. Ibrain. 2023. PMID: 38682019 Free PMC article. Review.
-
Eye-hand coordination during upper limb motor tasks in individuals with or without a neurodevelopmental disorder: a systematic review.Front Neurol. 2025 Jun 25;16:1569438. doi: 10.3389/fneur.2025.1569438. eCollection 2025. Front Neurol. 2025. PMID: 40635700 Free PMC article.
References
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous