

SARS-CoV-2 Susceptibility and COVID-19 Mortality Among Older Adults With Cognitive Impairment: Cross-Sectional Analysis From Hospital Records in a Diverse US Metropolitan Area
- PMID: 34367054
- PMCID: PMC8344862
- DOI: 10.3389/fneur.2021.692662
SARS-CoV-2 Susceptibility and COVID-19 Mortality Among Older Adults With Cognitive Impairment: Cross-Sectional Analysis From Hospital Records in a Diverse US Metropolitan Area
Abstract
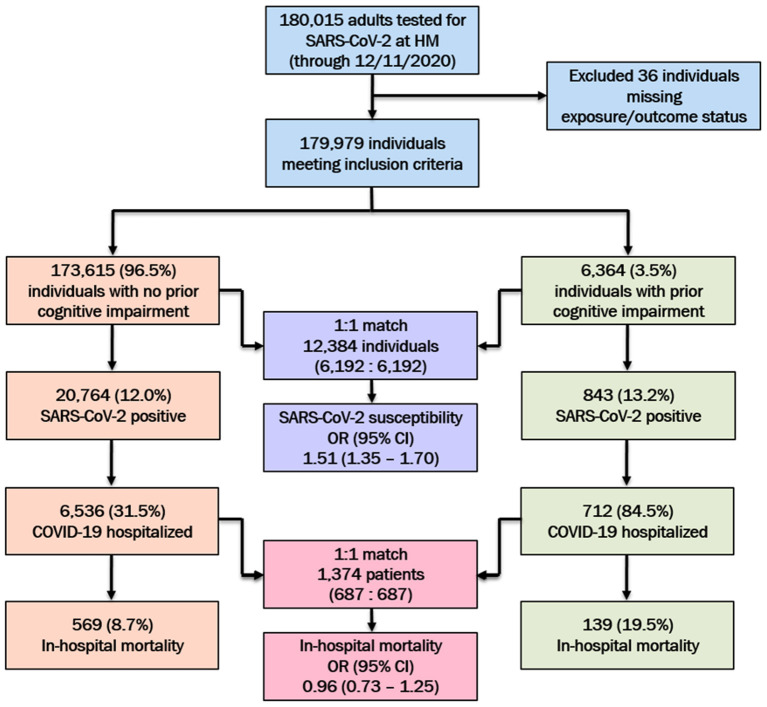
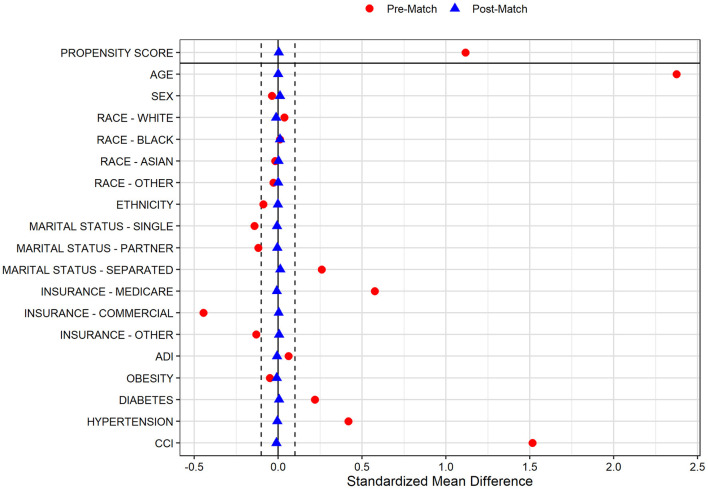
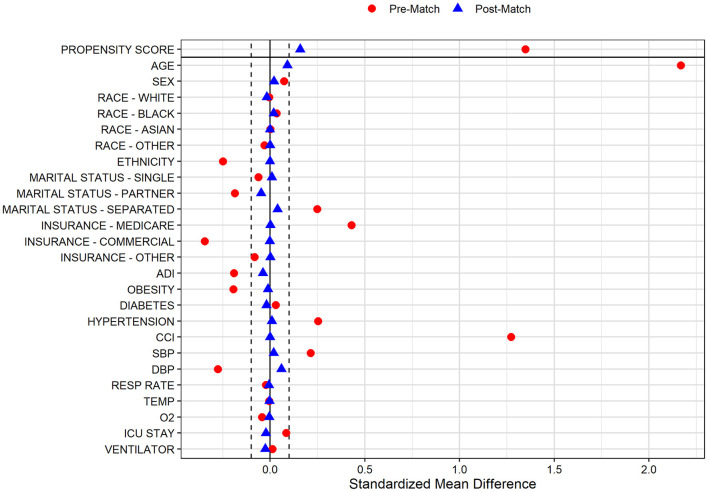
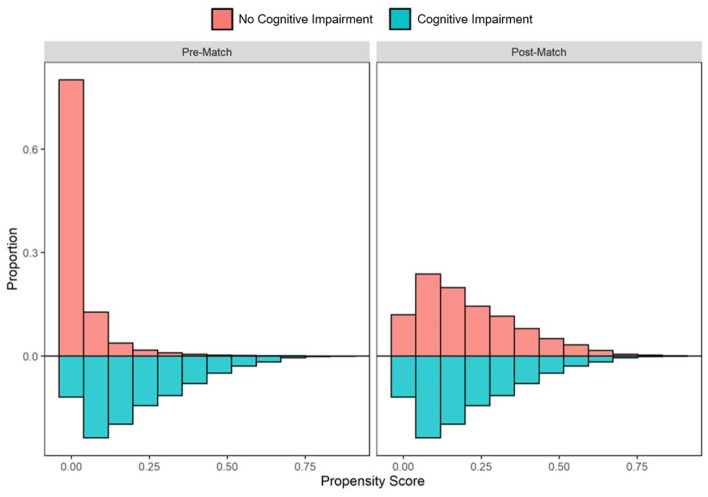
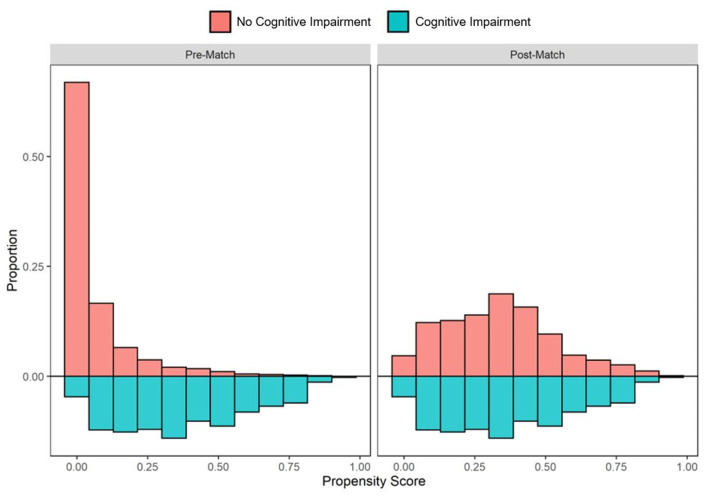
Introduction: Persistent knowledge gaps exist as to the extent that preexisting cognitive impairment is a risk factor for susceptibility to severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) and mortality from the coronavirus disease 2019 (COVID-19). Methods: We conducted a cross-sectional analysis of adults tested for SARS-CoV-2 at a tertiary healthcare system. Cognitive impairment was identified utilizing diagnosis codes (mild cognitive impairment, Alzheimer's disease, vascular, and other dementias) or cognitive impairment-specific medication use. Propensity score (PS) matched analyses were utilized to report odds ratios (OR) and 95% confidence intervals (CI) for association of cognitive impairment with SARS-CoV-2 susceptibility and COVID-19 mortality. Results: Between March-3rd and December-11th, 2020, 179,979 adults were tested, of whom 21,607 (12.0%) tested positive. We identified 6,364 individuals with preexisting cognitive impairment (mean age: 78.5 years, 56.8% females), among whom 843 (13.2%) tested positive and 139 (19.5%) of those hospitalized died. In the pre-PS matched cohort, cognitive impairment was significantly associated with increased SARS-CoV-2 susceptibility (OR, CI: 1.12, 1.04-1.21) and COVID-19 mortality (OR, CI: 2.54, 2.07-3.12). One-to-one matches were identified for 6,192 of 6,364 (97.3%) individuals with prior cognitive impairment and 687 of 712 (96.5%) hospitalized patients with prior cognitive impairment. In the fully balanced post-matched cohort, preexisting cognitive impairment was significantly associated with higher likelihood of SARS-CoV-2 infection (OR, CI: 1.51, 1.35-1.70); however, cognitive impairment did not confer higher risk of COVID-19 mortality (OR, CI: 0.96, 0.73-1.25). Discussion: To mitigate the effects of healthcare catastrophes such as the COVID-19 pandemic, strategies for targeted prevention and risk-stratified comorbidity management are warranted among the vulnerable sub-population living with cognitive impairment.
Keywords: Alzheimer's disease; COVID-19; SARS-CoV-2; cognitive impairment; dementia; patient registries; propensity score matching.
Copyright © 2021 Pan, Meeks, Potter, Masdeu, Seshadri, Smith, Ory and Vahidy.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Racial and ethnic disparities in SARS-CoV-2 pandemic: analysis of a COVID-19 observational registry for a diverse US metropolitan population.BMJ Open. 2020 Aug 11;10(8):e039849. doi: 10.1136/bmjopen-2020-039849. BMJ Open. 2020. PMID: 32784264 Free PMC article.
-
Sex differences in susceptibility, severity, and outcomes of coronavirus disease 2019: Cross-sectional analysis from a diverse US metropolitan area.PLoS One. 2021 Jan 13;16(1):e0245556. doi: 10.1371/journal.pone.0245556. eCollection 2021. PLoS One. 2021. PMID: 33439908 Free PMC article.
-
Testing the efficacy and safety of BIO101, for the prevention of respiratory deterioration, in patients with COVID-19 pneumonia (COVA study): a structured summary of a study protocol for a randomised controlled trial.Trials. 2021 Jan 11;22(1):42. doi: 10.1186/s13063-020-04998-5. Trials. 2021. PMID: 33430924 Free PMC article.
-
The Impact of SARS-CoV-2 on Stroke Epidemiology and Care: A Meta-Analysis.Ann Neurol. 2021 Feb;89(2):380-388. doi: 10.1002/ana.25967. Epub 2020 Dec 9. Ann Neurol. 2021. PMID: 33219563 Free PMC article.
-
Dementia Clinical Care in Relation to COVID-19.Curr Treat Options Neurol. 2022;24(1):1-15. doi: 10.1007/s11940-022-00706-7. Epub 2022 Feb 23. Curr Treat Options Neurol. 2022. PMID: 35221646 Free PMC article. Review.
Cited by
-
Delirium and Psychiatric Sequelae Associated to SARS-CoV-2 in Asymptomatic Patients With Psychiatric History and Mild Cognitive Impairment as Risk Factors: Three Case Reports.Front Psychiatry. 2022 Apr 7;13:868286. doi: 10.3389/fpsyt.2022.868286. eCollection 2022. Front Psychiatry. 2022. PMID: 35463530 Free PMC article.
-
Incidence and Outcomes of SARS-CoV-2 Infection in Older Adults Living with Dementia: A Population-Based Cohort Study.J Alzheimers Dis. 2022;89(2):681-693. doi: 10.3233/JAD-220369. J Alzheimers Dis. 2022. PMID: 35912744 Free PMC article.
-
Donepezil-associated survival benefits among Alzheimer's disease patients are retained but not enhanced during COVID-19 infections.Ther Adv Infect Dis. 2023 May 22;10:20499361231174289. doi: 10.1177/20499361231174289. eCollection 2023 Jan-Dec. Ther Adv Infect Dis. 2023. PMID: 37234745 Free PMC article.
-
Associations of cognitive impairment with self-isolation and access to health and care during the COVID-19 pandemic in England.Sci Rep. 2023 Mar 28;13(1):5026. doi: 10.1038/s41598-023-31241-3. Sci Rep. 2023. PMID: 36977759 Free PMC article.
-
Neuropathological Aspects of SARS-CoV-2 Infection: Significance for Both Alzheimer's and Parkinson's Disease.Front Neurosci. 2022 May 3;16:867825. doi: 10.3389/fnins.2022.867825. eCollection 2022. Front Neurosci. 2022. PMID: 35592266 Free PMC article. Review.
References
-
- Razzaghi H, Wang Y, Lu H, Marshall KE, Dowling NF, Paz-Bailey G, et al. . Estimated county-level prevalence of selected underlying medical conditions associated with increased risk for severe COVID-19 illness - United States, 2018. MMWR Morb Mortal Wkly Rep. (2020) 69:945–50. 10.15585/mmwr.mm6929a1 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous