

Incidence of Associated Lesions of Multiligament Knee Injuries: A Systematic Review and Meta-analysis
- PMID: 34368374
- PMCID: PMC8312178
- DOI: 10.1177/23259671211010409
Incidence of Associated Lesions of Multiligament Knee Injuries: A Systematic Review and Meta-analysis
Abstract
Background: The incidence of concomitant injuries, including meniscal and cartilage injuries, has not been adequately reported in previous studies on multiligament knee injury (MLKI) because their primary focal points have been the degree of ligament injury, treatment strategy, involvement of other soft tissues, and neurovascular injury.
Purpose: To analyze the incidence of associated lesions in MLKIs, including medial and lateral meniscal injuries, cartilage lesions, and complications.
Study design: Systemic review; Level of evidence, 4.
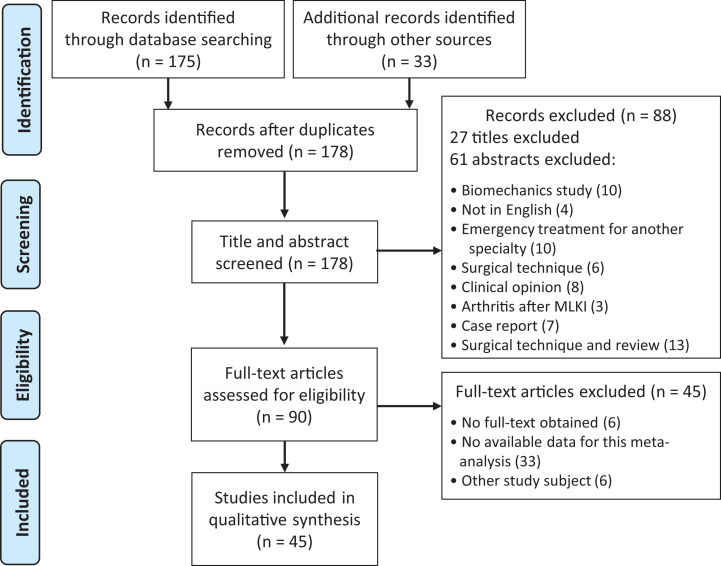
Methods: The PubMed, Embase, Cochrane Library, CINAHL, and Scopus databases were searched between inception and April 30, 2020. Studies were included if they reported the incidence rates of medial and/or lateral meniscal tears and cartilage injuries in cases of MLKIs. For the meta-analysis, data were extracted on clinical outcomes measured according to the number of medial and/or lateral meniscal tears, cartilage injuries, and complications.
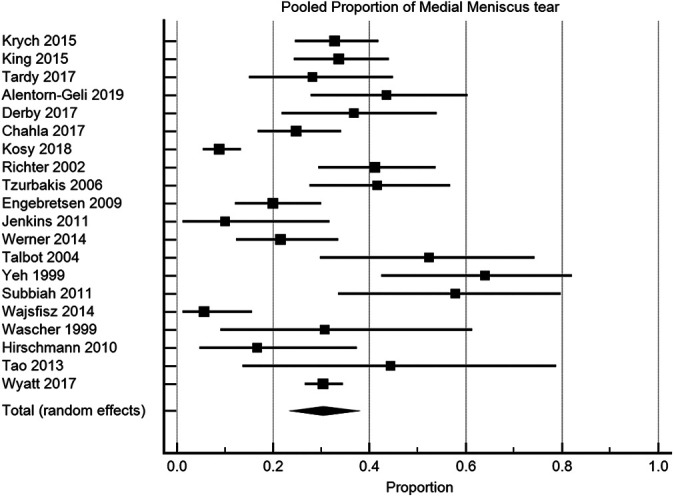
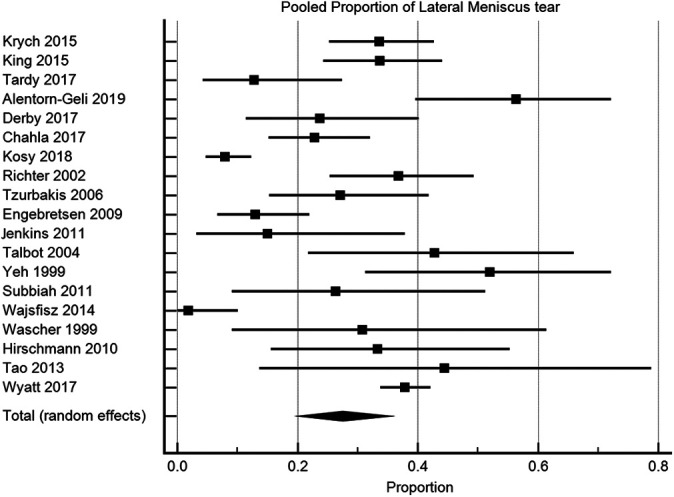
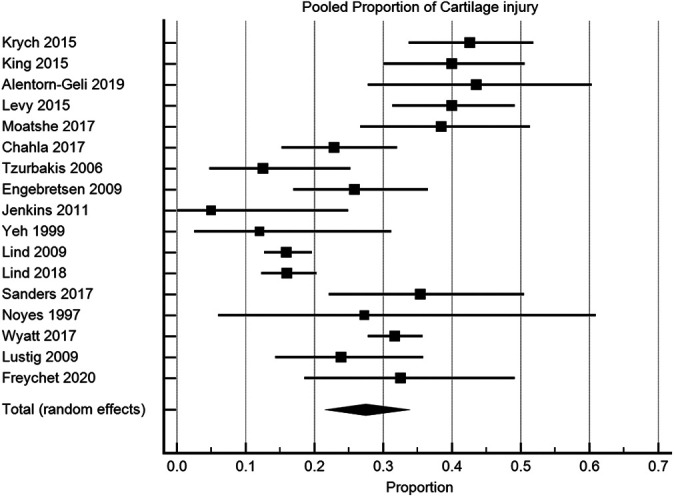
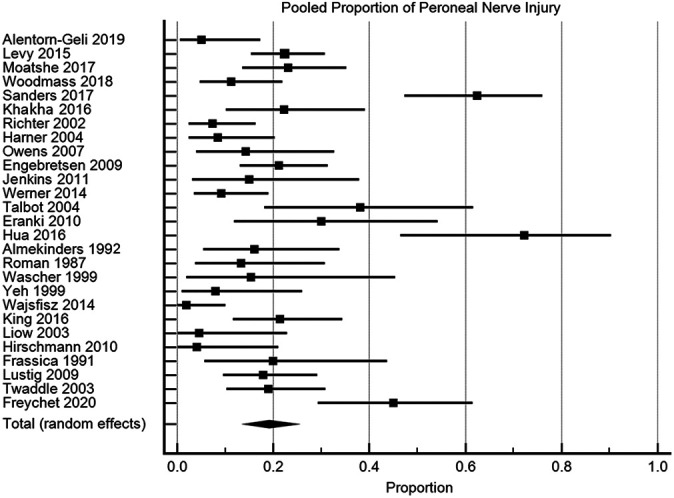
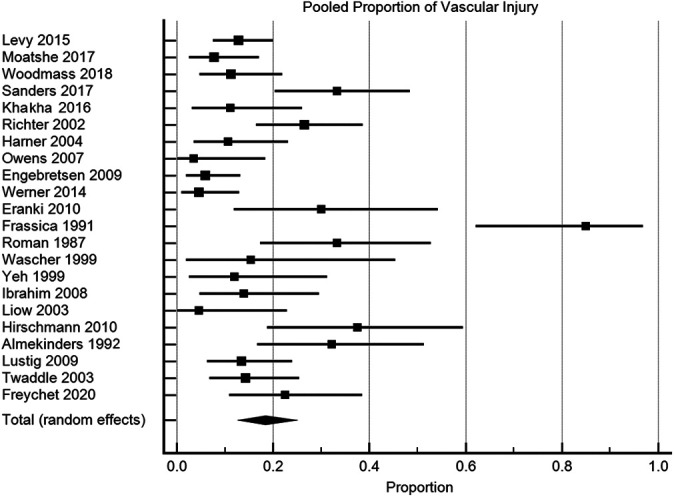
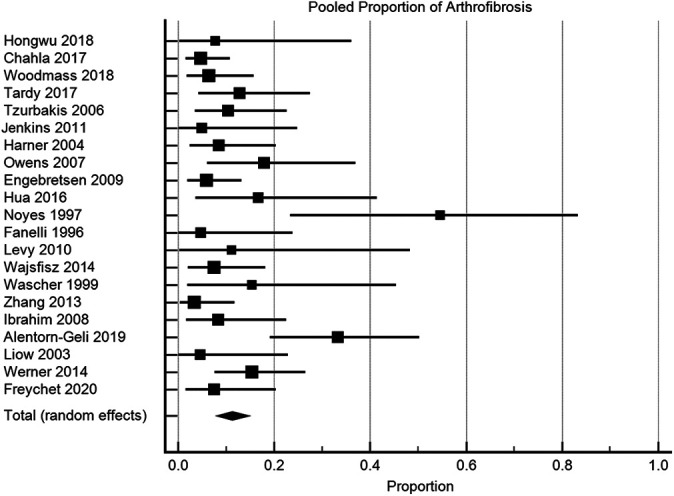
Results: A total of 45 studies were included in the MLKI analysis (3391 patients). The pooled rate of medial meniscal tears was 30.4% (95% CI, 24.1%-37.1%; P < .0001; I 2 = 85.8%). The pooled rate of lateral meniscal tears was 27.5% (95% CI, 20.3%-35.3%; P < .0001; I 2 = 89.6%). The pooled rate of cartilage injuries was 27.5% (95% CI, 22.1%-33.3%; P < .0001; I 2 = 86.8%). The pooled rates of peroneal nerve injuries, vascular injuries, and arthrofibrosis were 19.2% (95% CI, 14.2%-24.7%; P < .001; I 2 = 81.3%), 18.4% (95% CI, 13.2%-24.3%; P < .0001; I 2 = 81.0%), and 11.2% (95% CI, 8.1%-14.7%; P = .0018; I 2 = 54.0%), respectively.
Conclusion: The pooled rates of meniscal tears and cartilage injuries concomitant with MLKIs were high, ranging from 27% to 30%, and the pooled rates of peroneal nerve injury, vascular injury, and arthrofibrosis were considerable, ranging from 11% to 19%. The influence of these associated lesions on clinical results should be evaluated in future clinical studies.
Keywords: anterior cruciate ligament; cartilage; meniscus; meta-analysis; multiligament knee injury; outcomes.
© The Author(s) 2021.
Conflict of interest statement
One or more of the authors has declared the following potential conflict of interest or source of funding: This research was supported by a research grant from Chung-Ang University (2019). N.P. has received educational consulting fees from Smith & Nephew, LimaCorporate, Stryker, and Zimmer Biomet. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Figures
References
-
- Ahlén M, Lidén M. A comparison of the clinical outcome after anterior cruciate ligament reconstruction using a hamstring tendon autograft with special emphasis on the timing of the reconstruction. Knee Surg Sports Traumatol Arthrosc. 2011;19(3):488–494. - PubMed
-
- Ahn JH, Bae TS, Kang KS, Kang SY, Lee SH. Longitudinal tear of the medial meniscus posterior horn in the anterior cruciate ligament–deficient knee significantly influences anterior stability. Am J Sports Med. 2011;39(10):2187–2193. - PubMed
-
- Alentorn-Geli E, Lazarides AL, Utturkar GM, et al. Factors predictive of poorer outcomes in the surgical repair of multiligament knee injuries. Knee Surg Sports Traumatol Arthrosc. 2019;27(2):445–459. - PubMed
-
- Almekinders LC, Logan TC. Results following treatment of traumatic dislocations of the knee joint. Clin Orthop Relat Res. 1992;284:203–207. - PubMed
-
- Barfield WR, Holmes RE, Slone H, Walton ZJ, Hartsock LA. Acute versus staged surgical intervention in multiligamentous knee injuries: a review of the literature since 2009. Curr Orthop Pract. 2015;26(5):530–535.
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
