

Implications of Iron Deficiency in STEMI Patients and in a Murine Model of Myocardial Infarction
- PMID: 34368505
- PMCID: PMC8326269
- DOI: 10.1016/j.jacbts.2021.05.004
Implications of Iron Deficiency in STEMI Patients and in a Murine Model of Myocardial Infarction
Abstract
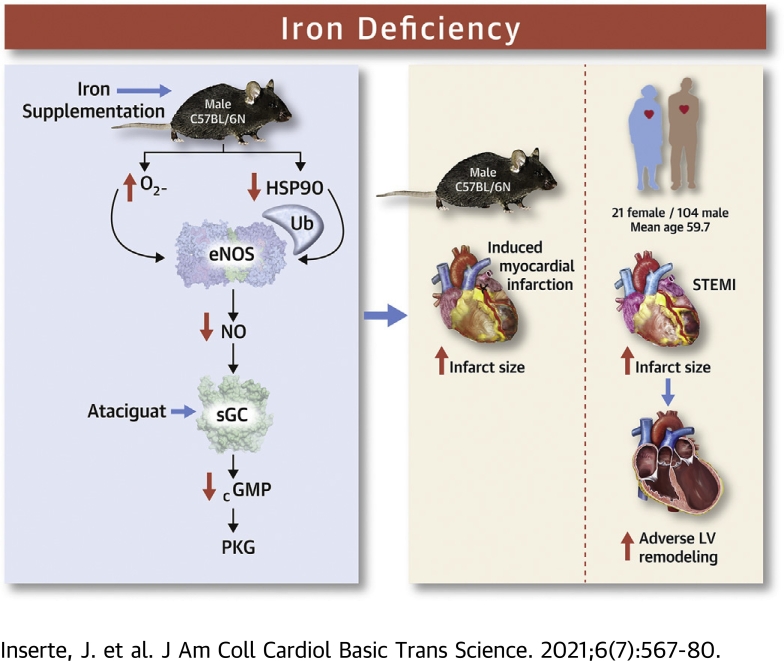
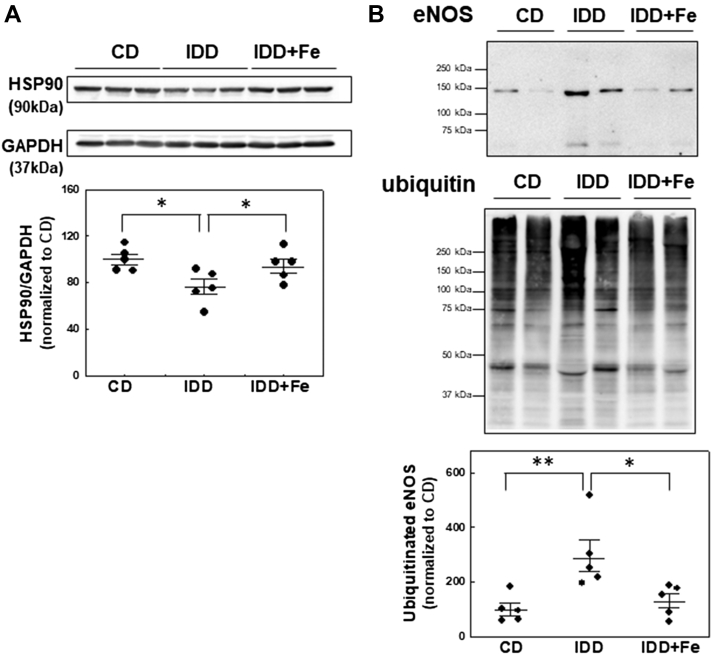
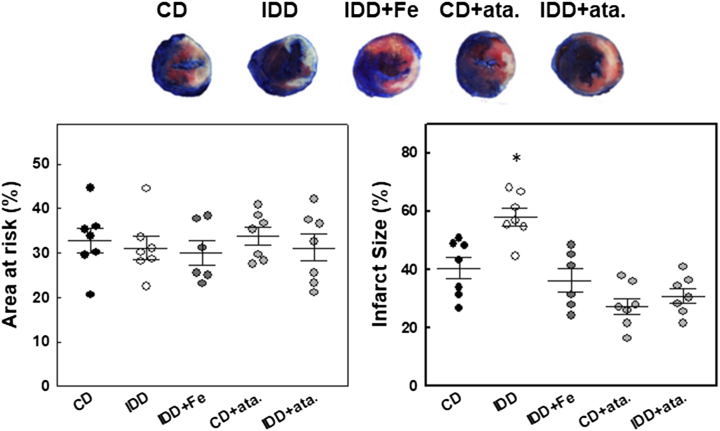
In patients with a first anterior ST-segment elevation myocardial infarction treated with primary percutaneous coronary intervention, iron deficiency (ID) was associated with larger infarcts, more extensive microvascular obstruction, and higher frequency of adverse left ventricular remodeling as assessed by cardiac magnetic resonance imaging. In mice, an ID diet reduced the activity of the endothelial nitric oxide synthase/soluble guanylate cyclase/protein kinase G pathway in association with oxidative/nitrosative stress and increased infarct size after transient coronary occlusion. Iron supplementation or administration of an sGC activator before ischemia prevented the effects of the ID diet in mice. Not only iron excess, but also ID, may have deleterious effects in the setting of ischemia and reperfusion.
Keywords: CK-MB, creatine kinase-myocardial band; CMR, cardiac magnetic resonance; HSP90, heat-shock protein 90; ID, iron deficiency; LV, left ventricular; MVO, microvascular obstruction; PKG, protein kinase G; STEMI, ST-segment elevation acute myocardial infarction; STIR, short tau inversion recovery; VASP, vasodilator-stimulated phosphoprotein; acute myocardial infarction; eNOS, endothelial nitric oxide synthase; endothelial nitric oxide synthase; iNOS, inducible nitric oxide synthase; iron deficiency; myocardial reperfusion; sGC, soluble guanylyl cyclase; soluble guanylate cyclase.
© 2021 The Authors.
Conflict of interest statement
This study was funded by Instituto de Salud Carlos III, Spain, through the project PI16/00232 and the research network CIBERCV (CB16/11/00479), both cofunded by European Regional Development Fund, and by the Sociedad Española de Cardiología (Proyecto de Investigación Traslacional en Cardiología 2016). The authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures
References
-
- Anker S.D., Comin Colet J., Filippatos G. Ferric carboxymaltose in patients with heart failure and iron deficiency. N Engl J Med. 2009;361:2436–2438. - PubMed
-
- Rocha B.M.L., Cunha G.J.L., Menezes Falcão L.F. The burden of iron deficiency in heart failure: therapeutic approach. J Am Coll Cardiol. 2018;71:782–793. - PubMed
-
- Meroño O., Cladellas M., Ribas-Barquet N. Iron deficiency is a determinant of functional capacity and health-related quality of life 30 days after an acute coronary syndrome. Rev Esp Cardiol. 2017;70:363–370. - PubMed
-
- González-D'Gregorio J., Miñana G., Núñez J. Iron deficiency and long-term mortality in elderly patients with acute coronary syndrome. Biomark Med. 2018;12:987–999. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
