

Ocular toxoplasmosis: a review of the current diagnostic and therapeutic approaches
- PMID: 34370174
- PMCID: PMC8351587
- DOI: 10.1007/s10792-021-01994-9
Ocular toxoplasmosis: a review of the current diagnostic and therapeutic approaches
Abstract
Purpose: This review aims to summarize the current knowledge concerning the clinical features, diagnostic work-up and therapeutic approach of ocular toxoplasmosis focusing mainly on the postnatally acquired form of the disease.
Methods: A meticulous literature search was performed in the PubMed database. A supplementary search was made in Google Scholar to complete the collected items.
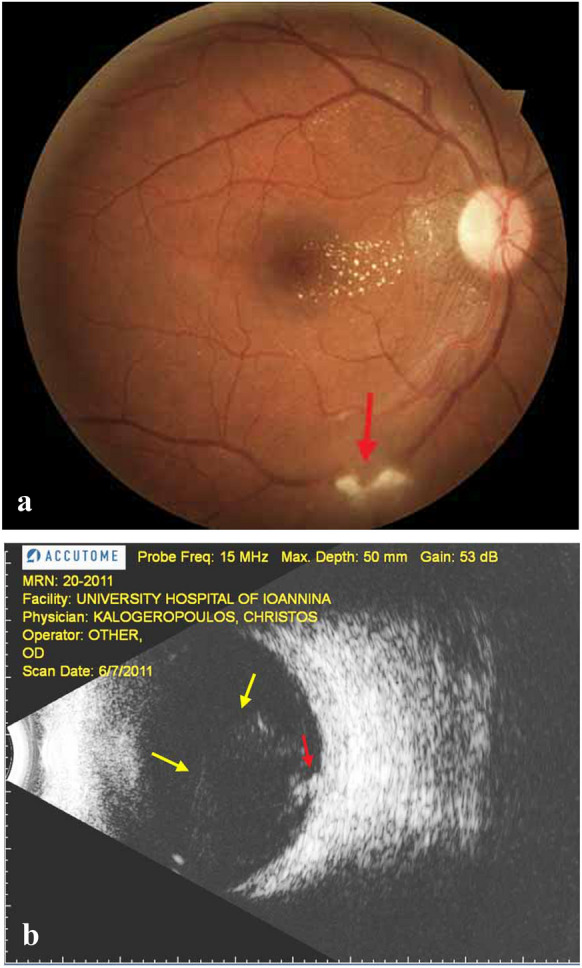
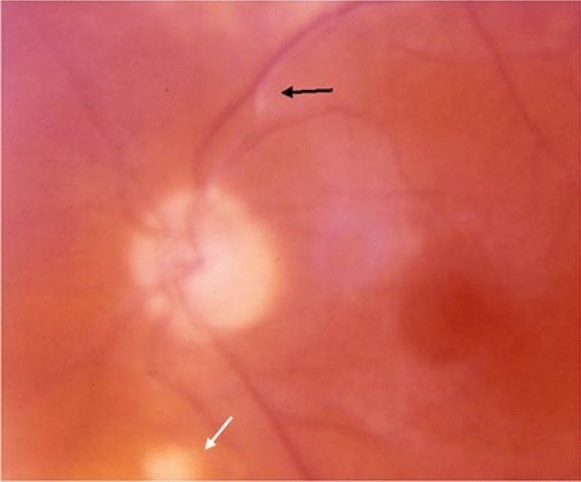
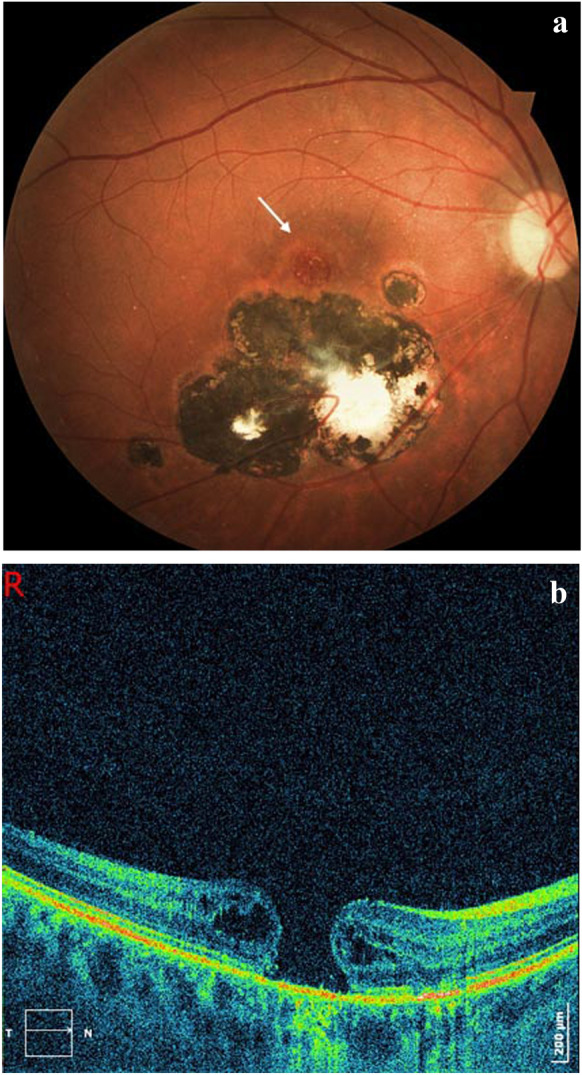
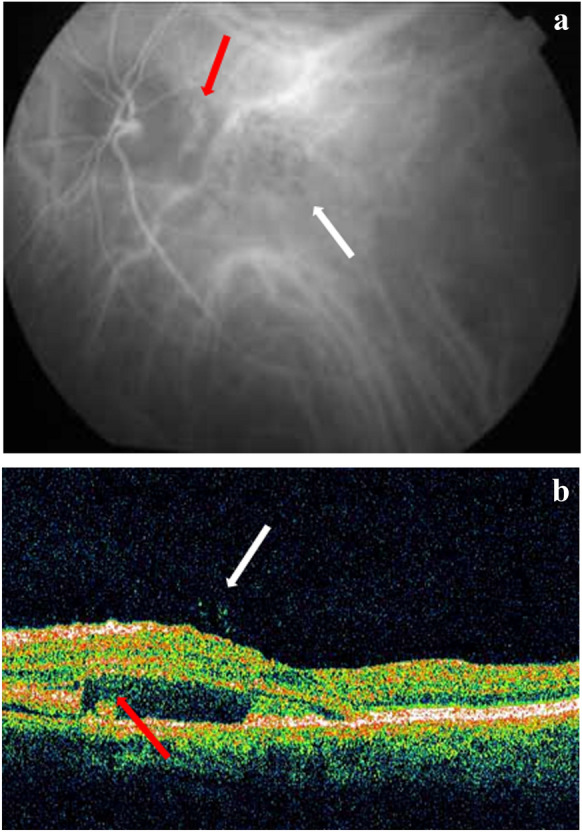
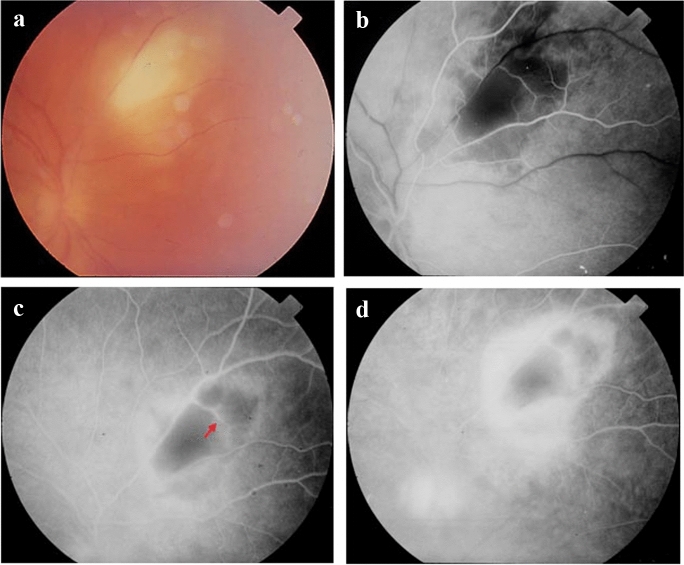
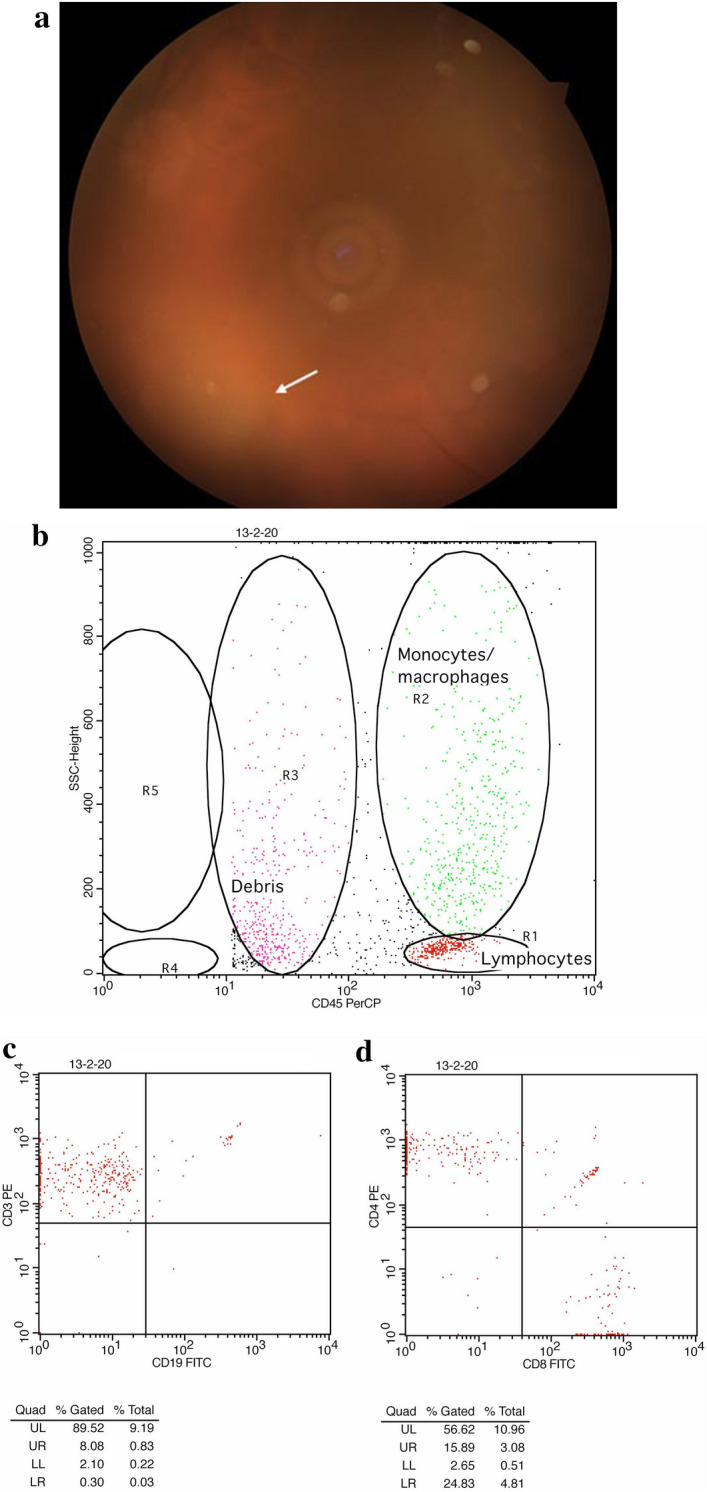
Results: Ocular toxoplasmosis is one of the most frequent infectious etiologies of posterior uveitis. It typically presents with retinochoroiditis. Setting an accurate diagnosis depends to a considerable degree on detecting characteristic clinical characteristics. In addition to the evaluation of clinical features, the diagnosis of toxoplasmosis relies at a large degree on serologic testing. The detection of the parasite DNA in the aqueous or vitreous humor can provide evidence for a definitive diagnosis. The current mainstay for the treatment, if necessary, is the use of oral antibiotic with systemic corticosteroids. Recent evidence suggests other therapeutic approaches, such as intravitreal antibiotics can be used.
Conclusion: Recent developments in the diagnostic and therapeutic approach have contributed to preventing or limiting vision loss of patients suffering from ocular toxoplasmosis. Further studies are required to provide a better understanding of epidemiology, pathogenesis, diagnosis, and treatment with a significant impact on the management of this challenging clinical entity.
Keywords: Ocular toxoplasmosis; Posterior uveitis; Retinochoroiditis; Toxoplasma gondii.
© 2021. The Author(s), under exclusive licence to Springer Nature B.V.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures

References
-
- Delair E, Latkany P et al (2011) Clinical manifestations of ocular toxoplasmosis. Ocul Immunol Inflamm 19(2):91–102. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
