

Self-reported exercise capacity among current smokers eligible for lung cancer screening: Distribution and association with key comorbidities
- PMID: 34371253
- PMCID: PMC8405582
- DOI: 10.1016/j.ctarc.2021.100443
Self-reported exercise capacity among current smokers eligible for lung cancer screening: Distribution and association with key comorbidities
Abstract
ONE CONCERN: as lung cancer screening (LCS) is implemented is that patients will be screened who are too ill to benefit. Poor exercise capacity (EC) predicts adverse outcomes following lung resection.
Objective: Describe the distribution of EC among smokers eligible for LCS and examine associations with comorbidities.
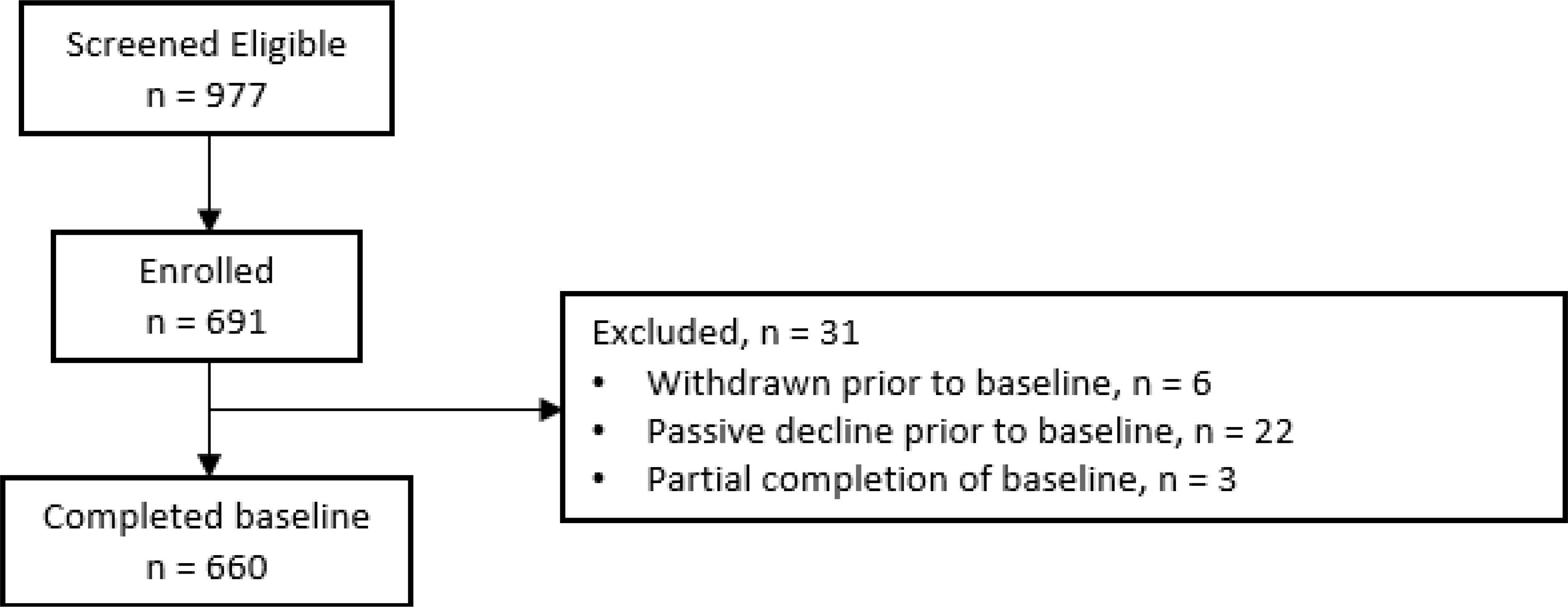
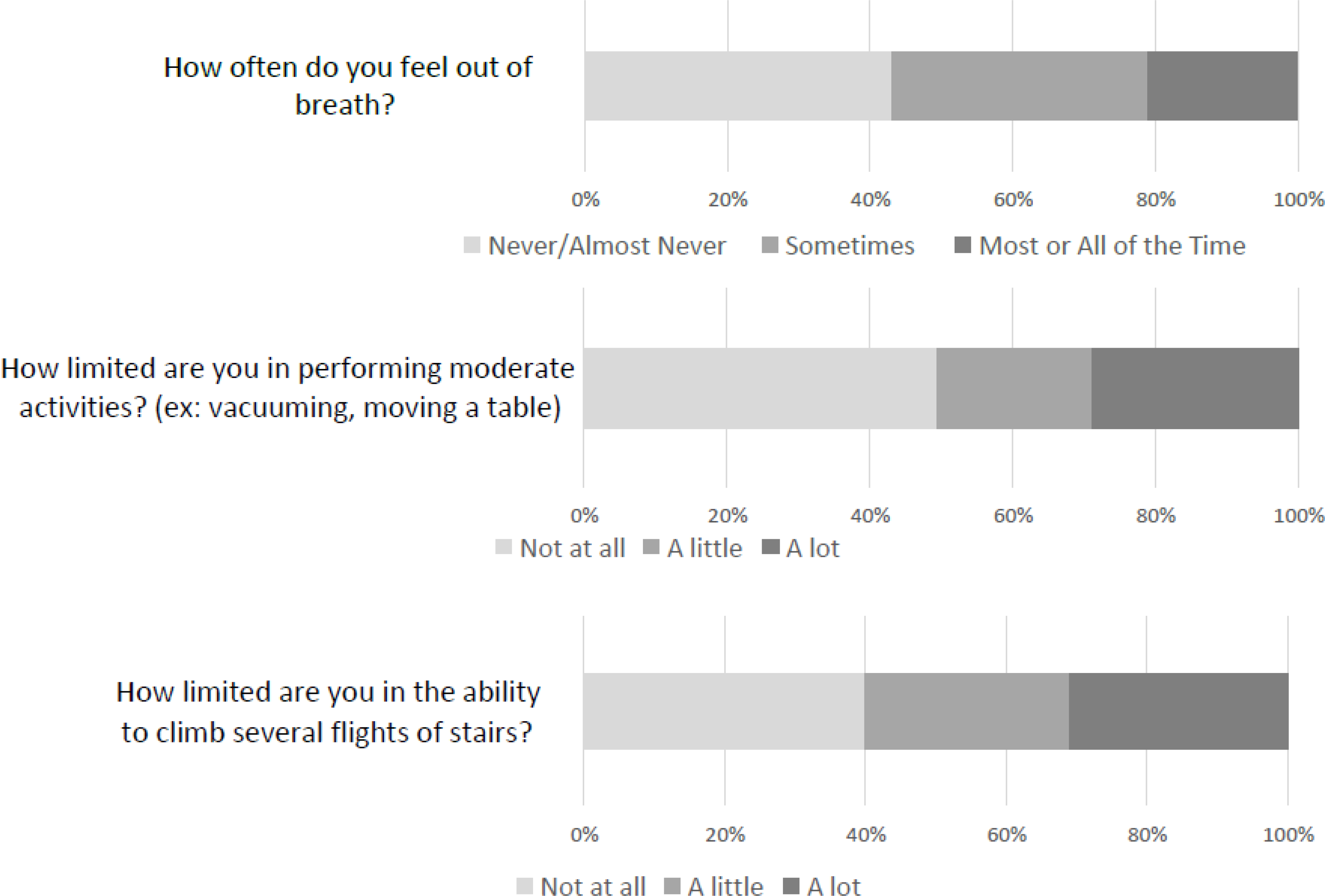
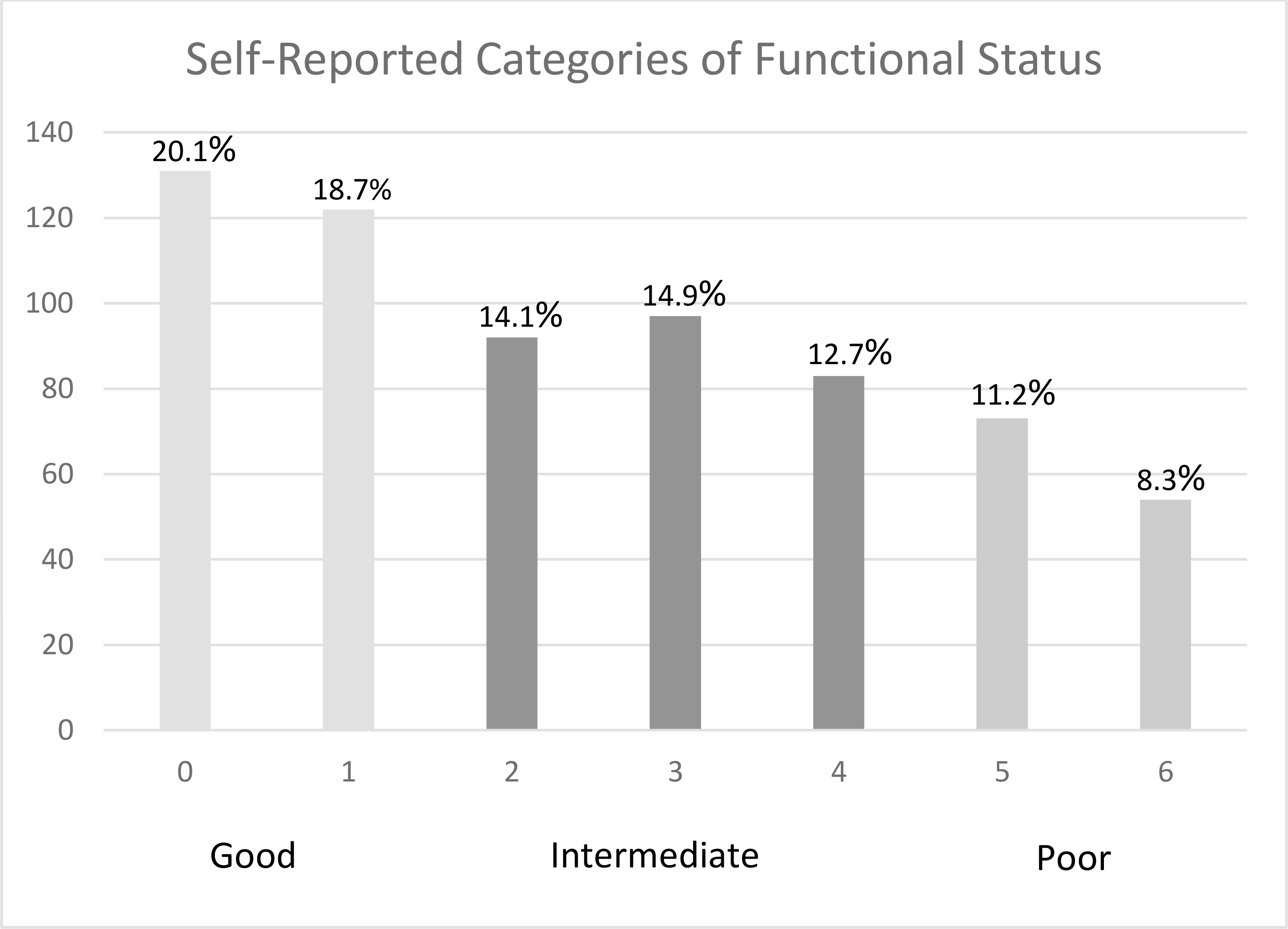
Methods: Cross-sectional analysis of baseline data from a randomized controlled trial of tobacco treatment in the context of LCS. Participants responded regarding limitations in moderate activities, ability to climb stairs, and frequency of dyspnea on a scale from never/almost never to all or most of the time. Responses were assigned a numeric score and summed to categorize exercise limitation. Associations between poor EC and key comorbidities were examined using adjusted logistic regression.
Results: 660 participants completed a survey with the following characteristics: 64.4% male, 89.5% white, mean age 64.5. Overall EC categories were: good 39.0%, intermediate 41.6%, and poor 19.4%. Prevalence of poor EC was higher among patients with COPD (OR 4.62 95%CI 3.05-7.02), heart failure (OR 3.07 95%CI 1.62-5.82) and cardiovascular disease (OR 2.24, 95%CI 1.45-3.47), and was highest among patients with multimorbidity. Among patients with COPD and heart failure, 57% had poor and 0% had good EC. In adjusted logistic regression, only COPD and Charlson comorbidity index remained significantly associated with poor EC.
Conclusions: Many patients eligible for LCS reported poor EC, with increased odds of poor EC among patients with comorbidities. More research is needed to determine how to best integrate EC and comorbidity into eligibility and shared decision-making conversations.
Keywords: Cancer screening; Comorbidity; Exercise capacity; Functional capacity; Lung cancer; Lung cancer screening; Multimorbidity.
Copyright © 2021. Published by Elsevier Ltd.
Conflict of interest statement
The authors report no conflicts of interest.
Declaration of interests
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
References
-
- Ou S-HI, Zell JA, Ziogas A and Anton-Culver H. Prognostic factors for survival of stage I nonsmall cell lung cancer patients. Cancer. 2007; 110: 1532–41. - PubMed
-
- Rivera MP, Tanner NT, Silvestri GA, et al.Incorporating Coexisting Chronic Illness into Decisions about Patient Selection for Lung Cancer Screening. An Official American Thoracic Society Research Statement. Am J Resp Crit Care Med. 2018; 198: e3–e13. - PubMed
-
- Desai H, Natt B, Kim S and Bime C. Decreased In-Hospital Mortality after Lobectomy Using Video-assisted Thoracoscopic Surgery Compared with Open Thoracotomy. Ann Am Thorac Soc. 2017; 14: 262–6. - PubMed
