

Low Bone Mineral Density and Risk for Osteoporotic Fractures in Patients with Chronic Pancreatitis
- PMID: 34371899
- PMCID: PMC8308495
- DOI: 10.3390/nu13072386
Low Bone Mineral Density and Risk for Osteoporotic Fractures in Patients with Chronic Pancreatitis
Abstract
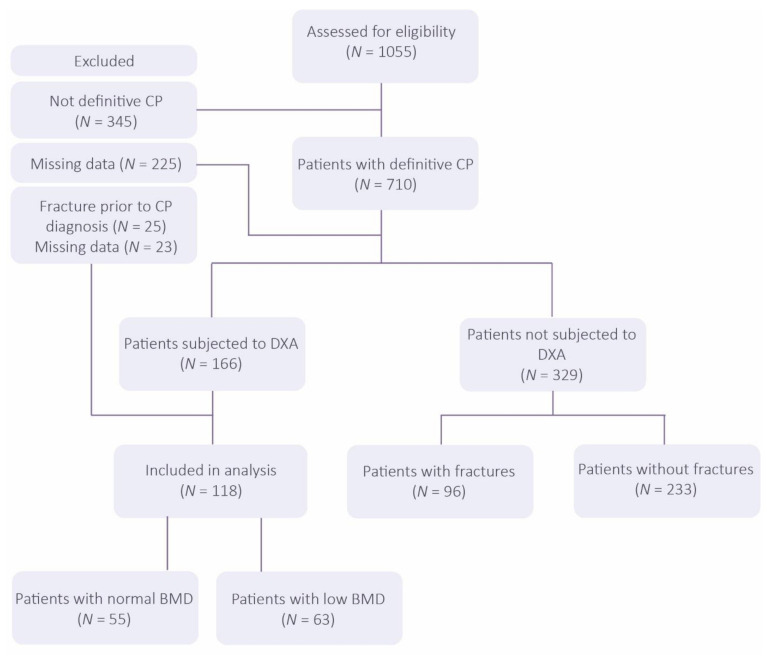
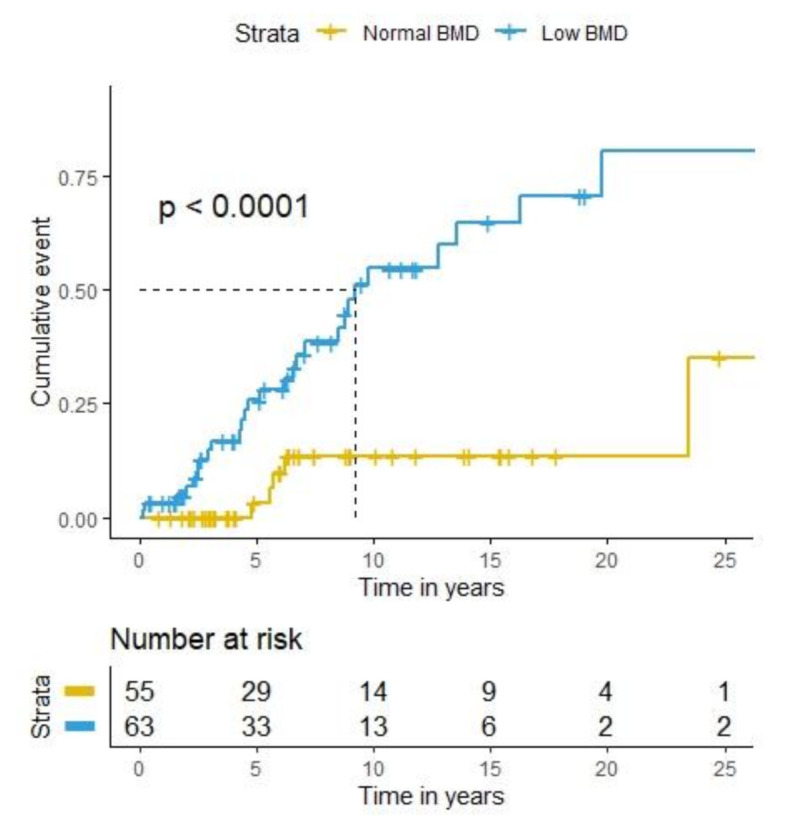
Introduction: Chronic pancreatitis (CP) can lead to malnutrition, an established risk factor for low bone mineral density (BMD) and fractures. This study aims to determine the prevalence of low BMD, assess fracture incidence and explore risk factors for fractures in patients with CP. Patients and methods: We performed a retrospective analysis of all patients treated for CP at Karolinska University Hospital between January 1999 and December 2020. Electronic medical records were retrieved to assess demographic, laboratory and clinical data. Patients subjected to dual-energy X-ray absorptiometry (DXA) were categorised as either low BMD or normal BMD. We investigated whether the rate of fractures, defined by chart review, differed between these groups using Cox regression, adjusting the model for age, sex and body mass index (BMI). Additional within-group survival analysis was conducted to identify potential risk factors. Results: DXA was performed in 23% of patients with definite CP. Some 118 patients were included in the final analysis. Low BMD was present in 63 (53.4%) patients. Mean age at CP diagnosis in the total cohort was 53.1 years and was significantly lower in patients with normal BMD than in patients with low BMD (45.5 vs. 59.8, p < 0.001). Significant differences were observed in smoking status and disease aetiology, i.e., a higher proportion of patients with low BMD were current or former smokers, with nicotine or alcohol being a more common cause of CP (p < 0.05). Total follow-up time was 898 person-years. Fractures were found in 33 (28.0%) patients: in 5 of 55 patients (16.7%) with normal DXA and in 28 of 63 patients (44.4%) with low BMD (adjusted hazard ratio = 3.4, 95% confidence interval (CI) = 1.2-9.6). Patients with at least 3 months of consecutive pancreatic enzyme replacement therapy (PERT) or vitamin D treatment had a longer median time to fracture after CP diagnosis. Conclusion: DXA was only performed in 23% of patients with definite CP in this study, indicating a low adherence to current European guidelines. A low BMD was found in 53.4% of patients with CP, and 44% of the patients with a low BMD experienced a fracture during follow-up. Moreover, the fracture rate in patients with low BMD increased compared to those with normal BMD.
Keywords: PERT; bone mineral density; chronic pancreatitis; fracture; osteoporosis.
Conflict of interest statement
M.K.,E.A., L.N.D., A.D., W.R., H.H., M.S., I.D.: none. M.V.: lecture fees Mylan, Abbott. J.-M.L.: lecture fees Mylan, Abbott. The authors declare no conflict of interest regarding the present study.
Figures
References
-
- Löhr J.M., Dominguez-Munoz E., Rosendahl J., Besselink M., Mayerle J., Lerch M.M., Haas S., Akisik F., Kartalis N., Iglesias-Garcia J., et al. United european gastroenterology evidence-based guidelines for the diagnosis and therapy of chronic pancreatitis (hapaneu) United Eur. Gastroenterol. J. 2017;5:153–199. doi: 10.1177/2050640616684695. - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
