

Investigation of SARS-CoV-2 faecal shedding in the community: a prospective household cohort study (COVID-LIV) in the UK
- PMID: 34372788
- PMCID: PMC8352155
- DOI: 10.1186/s12879-021-06443-7
Investigation of SARS-CoV-2 faecal shedding in the community: a prospective household cohort study (COVID-LIV) in the UK
Abstract
Background: SARS-CoV-2 is frequently shed in the stool of patients hospitalised with COVID-19. The extent of faecal shedding of SARS-CoV-2 among individuals in the community, and its potential to contribute to spread of disease, is unknown.
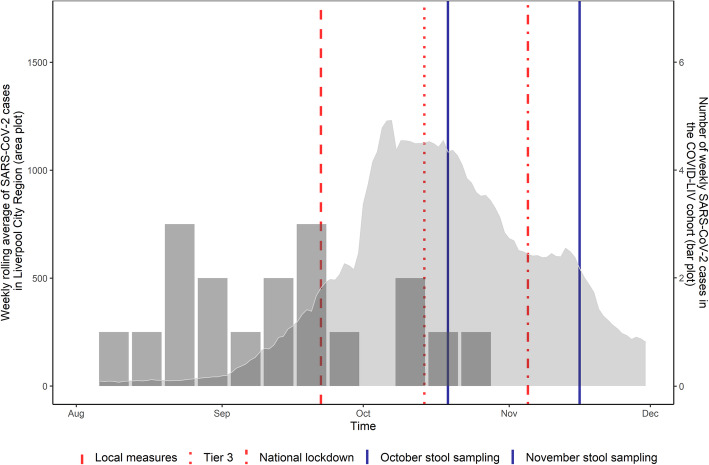
Methods: In this prospective, observational cohort study among households in Liverpool, UK, participants underwent weekly nasal/throat swabbing to detect SARS-CoV-2 virus, over a 12-week period from enrolment starting July 2020. Participants that tested positive for SARS-CoV-2 were asked to provide a stool sample three and 14 days later. In addition, in October and November 2020, during a period of high community transmission, stool sampling was undertaken to determine the prevalence of SARS-CoV-2 faecal shedding among all study participants. SARS-CoV-2 RNA was detected using Real-Time PCR.
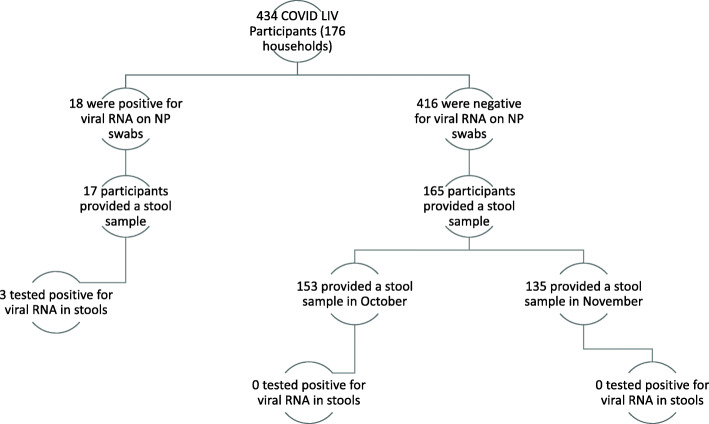
Results: A total of 434 participants from 176 households were enrolled. Eighteen participants (4.2%: 95% confidence interval [CI] 2.5-6.5%) tested positive for SARS-CoV-2 virus on nasal/throat swabs and of these, 3/17 (18%: 95% CI 4-43%) had SARS-CoV-2 detected in stool. Two of three participants demonstrated ongoing faecal shedding of SARS-CoV-2, without gastrointestinal symptoms, after testing negative for SARS-CoV-2 in respiratory samples. Among 165/434 participants without SARS-CoV-2 infection and who took part in the prevalence study, none had SARS-CoV-2 in stool. There was no demonstrable household transmission of SARS-CoV-2 among households containing a participant with faecal shedding.
Conclusions: Faecal shedding of SARS-CoV-2 occurred among community participants with confirmed SARS-CoV-2 infection. However, during a period of high community transmission, faecal shedding of SARS-CoV-2 was not detected among participants without SARS-CoV-2 infection. It is unlikely that the faecal-oral route plays a significant role in household and community transmission of SARS-CoV-2.
Keywords: Asymptomatic; COVID-19; Cohort study; Community; Faecal shedding; Gastrointestinal; SARS-CoV-2; Transmission.
© 2021. The Author(s).
Conflict of interest statement
NF reports research grant support from the Alder Hey Charity. MIG reports other financial or non-financial interests in V-PLEX Th17 Panel 1 Human Kit. LT reports research grant support from NIHR HPRU in Emerging and Zoonotic Infections related to this study. Unrelated to this study LT also reports fees paid to University of Liverpool from Eisai for providing a lecture on COVID-19 and cancer. WS reports scholarship for doctoral study at the University of Liverpool from the Ministry of Finance, Republic of Indonesia through the Indonesia Endowment Fund for Education program. DH, NAC, ERA, TS, KS and NMV have nothing to disclose.
Figures
References
-
- World Health Organization (WHO). Timeline of WHO’s response to COVID-19. https://www.who.int/emergencies/diseases/novel-coronavirus-2019/interact.... Accessed 2020 Nov 1.
-
- Wang D, Hu B, Hu C, Zhu F, Liu X, Zhang J, Wang B, Xiang H, Cheng Z, Xiong Y, Zhao Y, Li Y, Wang X, Peng Z. Clinical characteristics of 138 hospitalized patients with 2019 novel coronavirus–infected pneumonia in Wuhan, China. JAMA. 2020;323(11):1061–1069. doi: 10.1001/jama.2020.1585. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
