

Under-recognition of heart failure in patients with atrial fibrillation and the impact of gender: a UK population-based cohort study
- PMID: 34372832
- PMCID: PMC8353868
- DOI: 10.1186/s12916-021-02048-8
Under-recognition of heart failure in patients with atrial fibrillation and the impact of gender: a UK population-based cohort study
Abstract
Background: Patients with atrial fibrillation (AF) complicated by heart failure (HF) have a poor prognosis. We investigated whether long term loop-diuretic therapy in patients with AF and no known diagnosis of HF, as a potential surrogate marker of undiagnosed HF, is also associated with worse outcomes.
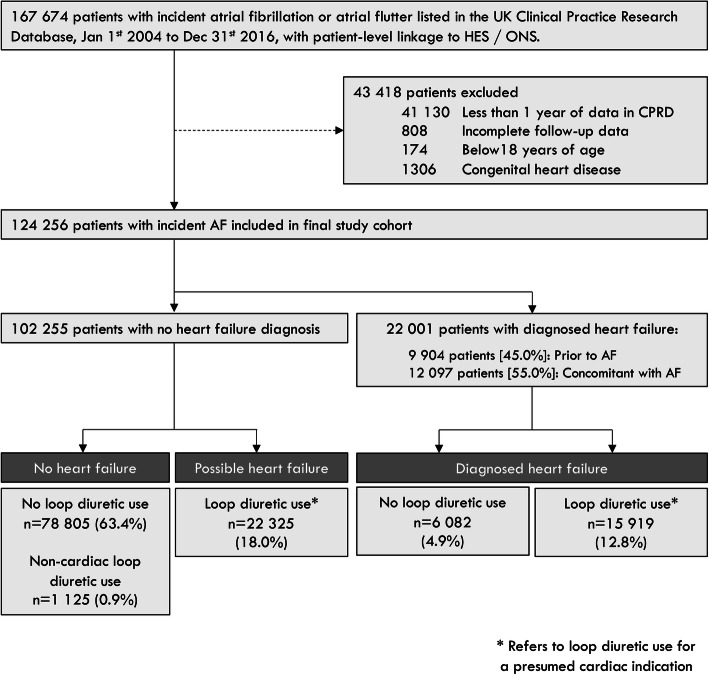
Methods: Adults with incident AF were identified from UK primary and secondary care records between 2004 and 2016. Repeat prescriptions for loop diuretics, without a diagnosis of HF or documented non-cardiac indication, were classified as 'isolated' loop diuretic use.
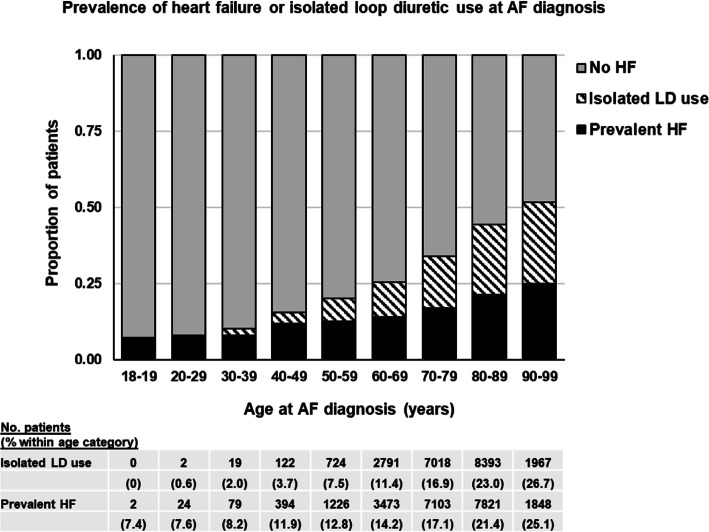
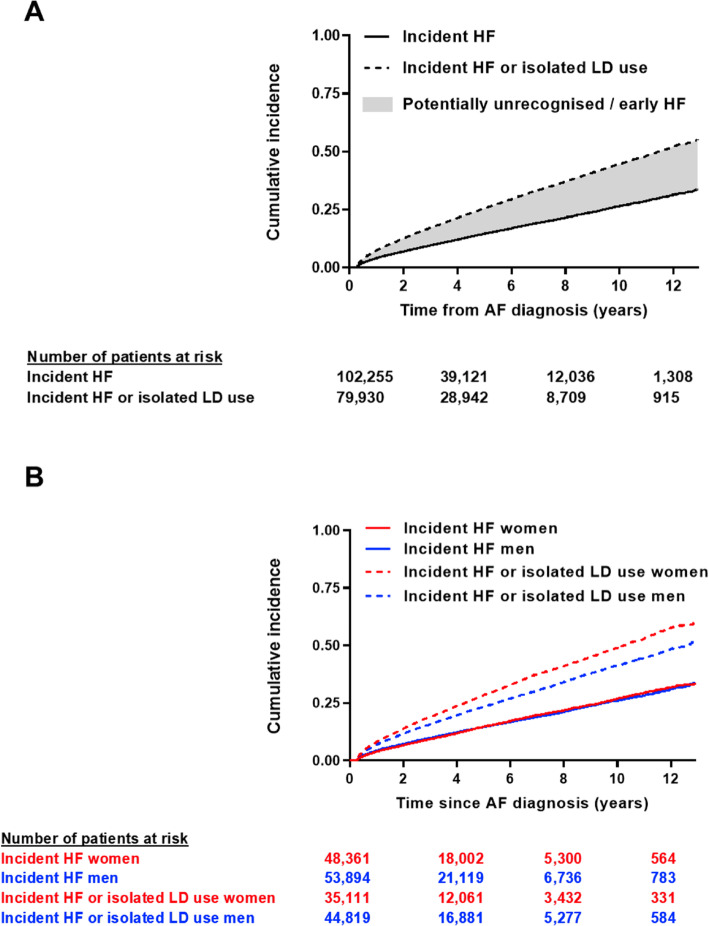
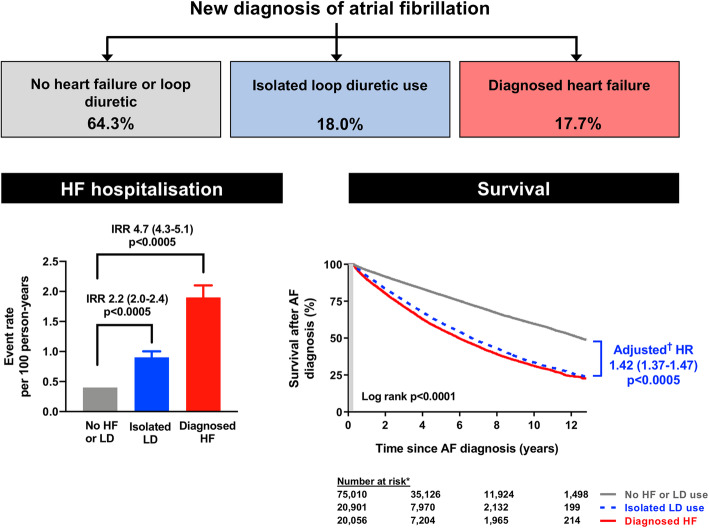
Results: Amongst 124,256 people with incident AF (median 76 years, 47% women), 22,001 (17.7%) had a diagnosis of HF, and 22,325 (18.0%) had isolated loop diuretic use. During 2.9 (LQ-UQ 1-6) years' follow-up, 12,182 patients were diagnosed with HF (incidence rate 3.2 [95% CI 3.1-3.3]/100 person-years). Of these, 3999 (32.8%) had prior isolated loop diuretic use, including 31% of patients diagnosed with HF following an emergency hospitalisation. The median time from AF to HF diagnosis was 3.6 (1.2-7.7) years in men versus 5.1 (1.8-9.9) years in women (p = 0.0001). In adjusted models, patients with isolated loop diuretic use had higher mortality (HR 1.42 [95% CI 1.37-1.47], p < 0.0005) and risk of HF hospitalisation (HR 1.60 [95% CI 1.42-1.80], p < 0.0005) than patients with no HF or loop diuretic use, and comparably poor survival to patients with diagnosed HF.
Conclusions: Loop diuretics are commonly prescribed to patients with AF and may indicate increased cardiovascular risk. Targeted evaluation of these patients may allow earlier HF diagnosis, timely intervention, and better outcomes, particularly amongst women with AF, in whom HF appears to be under-recognised and diagnosed later than in men.
Keywords: Atrial fibrillation; Epidemiology; Heart failure; Loop diuretics.
© 2021. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Ponikowski P, Voors AA, Anker SD, Bueno H, Cleland JGF, Coats AJS, Falk V, Gonzalez-Juanatey JR, Harjola VP, Jankowska EA, Jessup M, Linde C, Nihoyannopoulos P, Parissis JT, Pieske B, Riley JP, Rosano GMC, Ruilope LM, Ruschitzka F, Rutten FH, van der Meer P, Group ESCSD 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: the Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC)Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur Heart J. 2016;37(27):2129–2200. doi: 10.1093/eurheartj/ehw128. - DOI - PubMed
-
- van Doorn S, Geersing GJ, Kievit RF, van Mourik Y, Bertens LC, van Riet EES, Boonman-de Winter LJ, Moons KGM, Hoes AW, Rutten FH. Opportunistic screening for heart failure with natriuretic peptides in patients with atrial fibrillation: a meta-analysis of individual participant data of four screening studies. Heart. 2018;104(15):1236–1237. doi: 10.1136/heartjnl-2017-312781. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
