

The cytokines HGF and CXCL13 predict the severity and the mortality in COVID-19 patients
- PMID: 34373466
- PMCID: PMC8352963
- DOI: 10.1038/s41467-021-25191-5
The cytokines HGF and CXCL13 predict the severity and the mortality in COVID-19 patients
Abstract
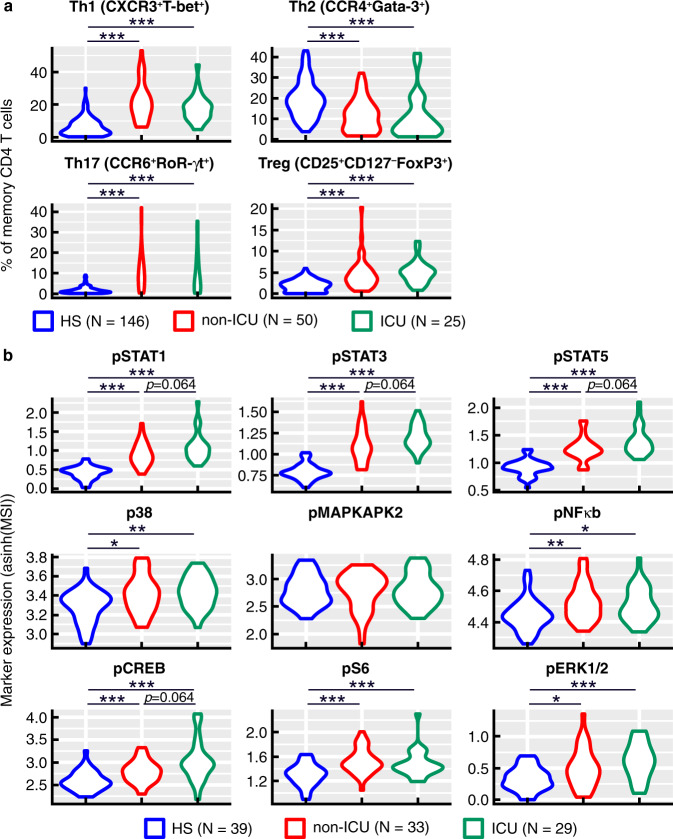
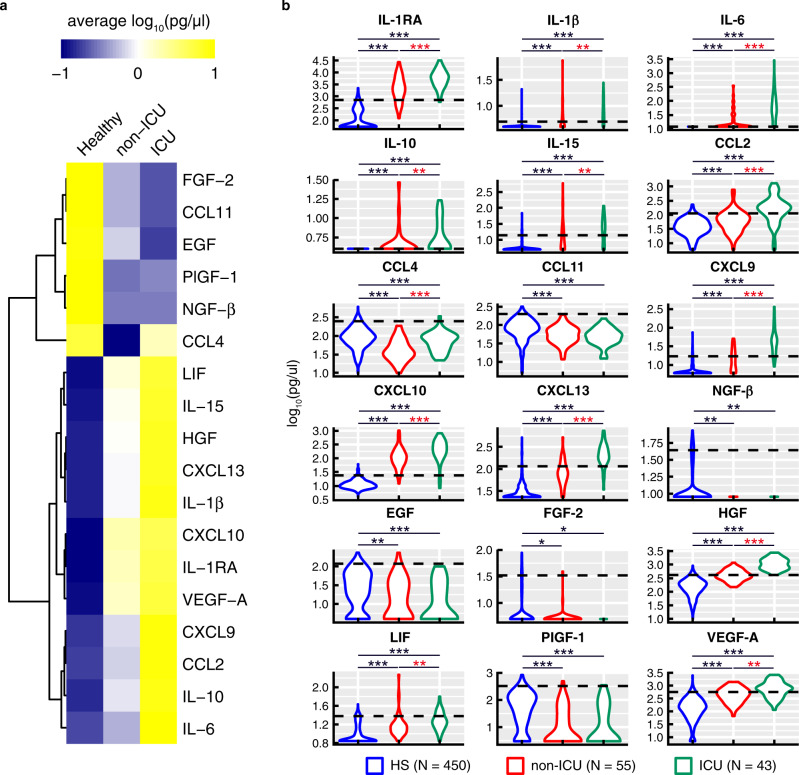
The objective of the present study was to identify biological signatures of severe coronavirus disease 2019 (COVID-19) predictive of admission in the intensive care unit (ICU). Over 170 immunological markers were investigated in a 'discovery' cohort (n = 98 patients) of the Lausanne University Hospital (LUH-1). Here we report that 13 out of 49 cytokines were significantly associated with ICU admission in the three cohorts (P < 0.05 to P < 0.001), while cellular immunological markers lacked power in discriminating between ICU and non-ICU patients. The cytokine results were confirmed in two 'validation' cohorts, i.e. the French COVID-19 Study (FCS; n = 62) and a second LUH-2 cohort (n = 47). The combination of hepatocyte growth factor (HGF) and C-X-C motif chemokine ligand 13 (CXCL13) was the best predictor of ICU admission (positive and negative predictive values ranging from 81.8% to 93.1% and 85.2% to 94.4% in the 3 cohorts) and occurrence of death during patient follow-up (8.8 fold higher likelihood of death when both cytokines were increased). Of note, HGF is a pleiotropic cytokine with anti-inflammatory properties playing a fundamental role in lung tissue repair, and CXCL13, a pro-inflammatory chemokine associated with pulmonary fibrosis and regulating the maturation of B cell response. Up-regulation of HGF reflects the most powerful counter-regulatory mechanism of the host immune response to antagonize the pro-inflammatory cytokines including CXCL13 and to prevent lung fibrosis in COVID-19 patients.
© 2021. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
