

Repeatability and comparability of the Galilei-G4 and Cassini in measuring corneal power and astigmatism in normal and post-refractive surgery eyes
- PMID: 34373485
- PMCID: PMC8352897
- DOI: 10.1038/s41598-021-94319-w
Repeatability and comparability of the Galilei-G4 and Cassini in measuring corneal power and astigmatism in normal and post-refractive surgery eyes
Abstract
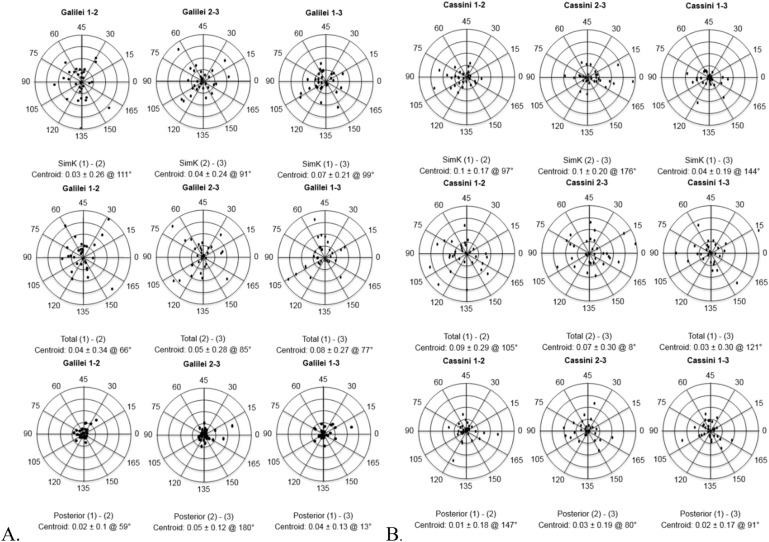
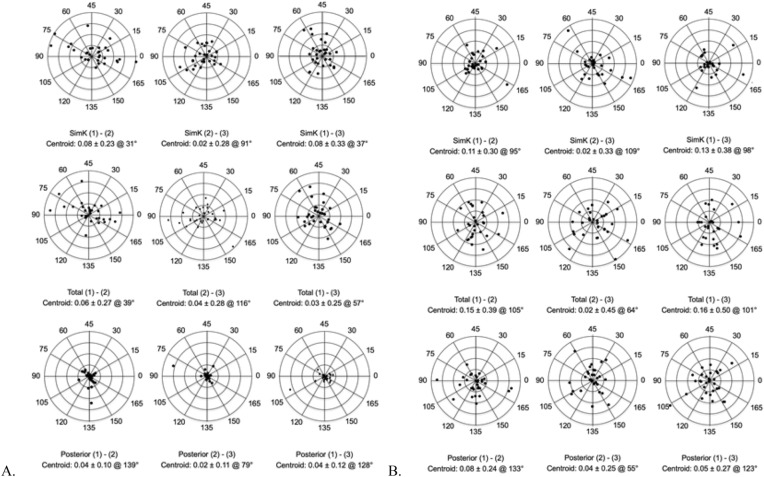
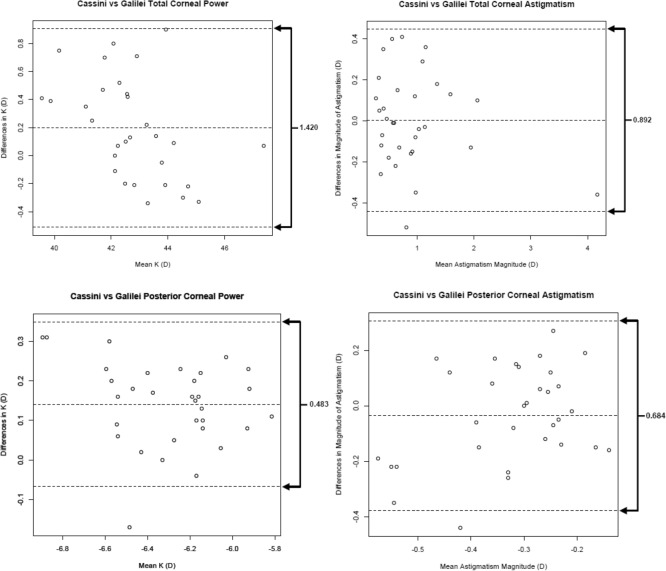
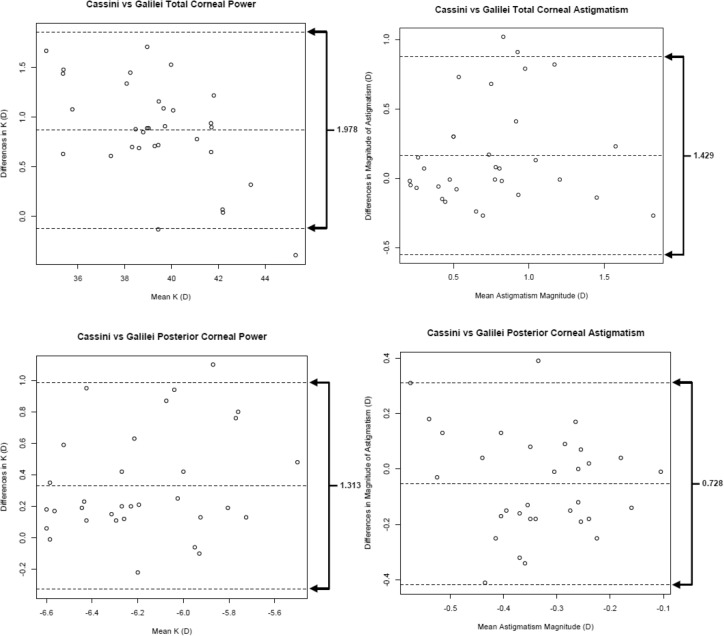
To assess the repeatability and comparability of the Galilei G4 versus the Cassini topographer in post-refractive eyes and in normal eyes, including older patients representative of an initial cataract evaluation. Simulated keratometric (simK), total corneal and posterior corneal power and astigmatism were evaluated in both post-refractive and normal eyes. Repeatability was measured by calculating within-subject standard deviation (Sw), coefficient of variation (CoV), and intraclass correlation coefficient (ICC). Vector analyses and Bland-Altman plots were employed to assess agreement between devices. We studied 32 subjects with a history of refractive surgery and 32 subjects without a history of refractive surgery undergoing cataract surgery. The mean age was 55 ± 18.5 years and the age range was 21.5-91.5 years. In non-refractive and post-refractive eyes, the ICC was > 0.9 (P < 0.001) for all corneal powers and for simK and total corneal astigmatism for both analyzers. The ICC for posterior corneal astigmatism magnitude using the Galilei was 0.62 and 0.67 and for the Cassini 0.55 and 0.38 in normal and post-refractive eyes, respectively. In both post-refractive and normal eyes, the Galilei G4 and Cassini analyzers have high repeatability in simK, total, and posterior corneal power and low repeatability for posterior corneal astigmatism.
© 2021. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Juhas T, Kozak I, Hornak M. Corneal topography and LASIK. Europe PMC. 2003;59:98–104. - PubMed
-
- National Institute for Health and Care Excellence (UK). Cataracts in adults: Management (National Institute for Health and Care Excellence (UK), London, 2017). (NICE Guideline, No. 77.) 7, Preoperative assessment and biometry. Available from: https://www.ncbi.nlm.nih.gov/books/NBK536589/. - PubMed
-
- Ventura BV, Al-Mohtaseb ZN, Wang L, Koch DD, Weikert MP. Repeatability and comparability of corneal power and corneal astigmatism obtained from a point-source color light-emitting diode topographer, a Placido-based corneal topographer, and a low-coherence reflectometer. Cataract Refract. Surg. 2015;41:2242–2250. doi: 10.1016/j.jcrs.2015.11.003. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
