

Screening outcomes by risk factor and age: evidence from BreastScreen WA for discussions of risk-stratified population screening
- PMID: 34374095
- PMCID: PMC9290915
- DOI: 10.5694/mja2.51216
Screening outcomes by risk factor and age: evidence from BreastScreen WA for discussions of risk-stratified population screening
Abstract
Objectives: To estimate rates of screen-detected and interval breast cancers, stratified by risk factor, to inform discussions of risk-stratified population screening.
Design: Retrospective population-based cohort study; analysis of routinely collected BreastScreen WA program clinical and administrative data.
Setting, participants: All BreastScreen WA mammography screening episodes for women aged 40 years or more during 1 July 2007 - 30 June 2017.
Main outcome measures: Cancer detection rate (CDR) and interval cancer rate (ICR), by risk factor.
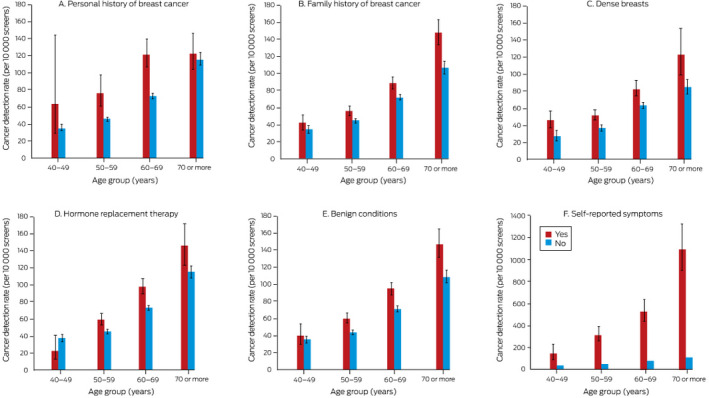
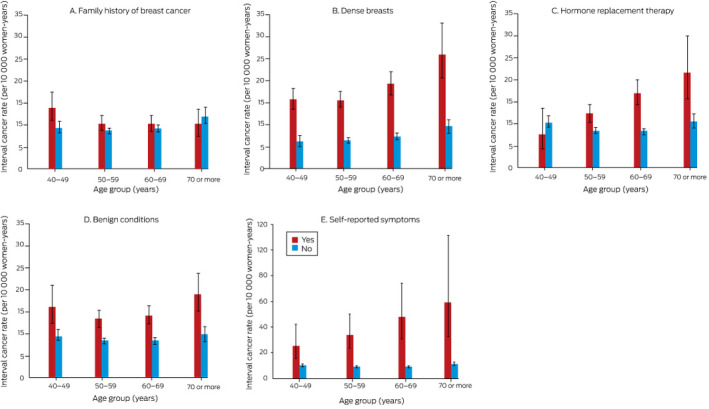
Results: A total of 323 082 women were screened in 1 026 137 screening episodes (mean age, 58.5 years; SD, 8.6 years). The overall CDR was 68 (95% CI, 67-70) cancers per 10 000 screens, and the overall ICR was 9.7 (95% CI, 9.2-10.1) cancers per 10 000 women-years. Interactions between the effects on CDR of age group and five risk factors were statistically significant: personal history of breast cancer (P = 0.039), family history of breast cancer (P = 0.005), risk-relevant benign conditions (P = 0.012), hormone-replacement therapy (P = 0.002), and self-reported symptoms (P < 0.001). The influence of these risk factors (except personal history) increased with age. For ICR, only the interaction between age and hormone-replacement therapy was significant (P < 0.001), although weak interactions between age and family history of breast cancer or having dense breasts were noted (each P = 0.07). The influence of family history on ICR was significant only for women aged 40-49 years.
Conclusions: Screening CDR and (for some risk factors) ICR were higher for women in some age groups with personal histories of breast cancer or risk-relevant benign breast conditions or first degree family history of breast cancer, women with dense breasts or self-reported breast-related symptoms, and women using hormone-replacement therapy. Our findings could inform the evaluation of risk-based screening.
Keywords: Breast neoplasms; Epidemiology; Mammography; Mass screening; Population health; Risk factors.
© 2021 The Authors. Medical Journal of Australia published by John Wiley & Sons Australia, Ltd on behalf of AMPCo Pty Ltd.
Conflict of interest statement
No relevant disclosures.
Figures
Comment in
-
Towards risk-stratified population breast cancer screening: more than mammographic density.Med J Aust. 2021 Oct 18;215(8):350-351. doi: 10.5694/mja2.51268. Epub 2021 Sep 16. Med J Aust. 2021. PMID: 34532866 No abstract available.
References
-
- Myers ER, Moorman P, Gierisch JM, et al. Benefits and harms of breast cancer screening: a systematic review. JAMA 2015; 314: 1615–1634. - PubMed
-
- Australian Institute of Health and Welfare . BreastScreen Australia monitoring report 2018 (Cat. no. CAN 116; Cancer Series no. 112). Updated 2 Oct 2018. https://www.aihw.gov.au/reports/cancer/breastscreen‐australia‐monitoring... (viewed Apr 2021).
-
- Cancer Council . Roadmap for optimising screening in Australia: breast. Undated. https://www.cancer.org.au/about‐us/policy‐and‐advocacy/early‐detection‐p... (viewed Apr 2021).
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
