

Severe Acute Respiratory Syndrome Coronavirus 2 Viremia Is Associated With Coronavirus Disease 2019 Severity and Predicts Clinical Outcomes
- PMID: 34374761
- PMCID: PMC9070832
- DOI: 10.1093/cid/ciab686
Severe Acute Respiratory Syndrome Coronavirus 2 Viremia Is Associated With Coronavirus Disease 2019 Severity and Predicts Clinical Outcomes
Abstract
Background: Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) viral RNA (vRNA) is detected in the bloodstream of some patients with coronavirus disease 2019 (COVID-19), but it is not clear whether this RNAemia reflects viremia (ie, virus particles) and how it relates to host immune responses and outcomes.
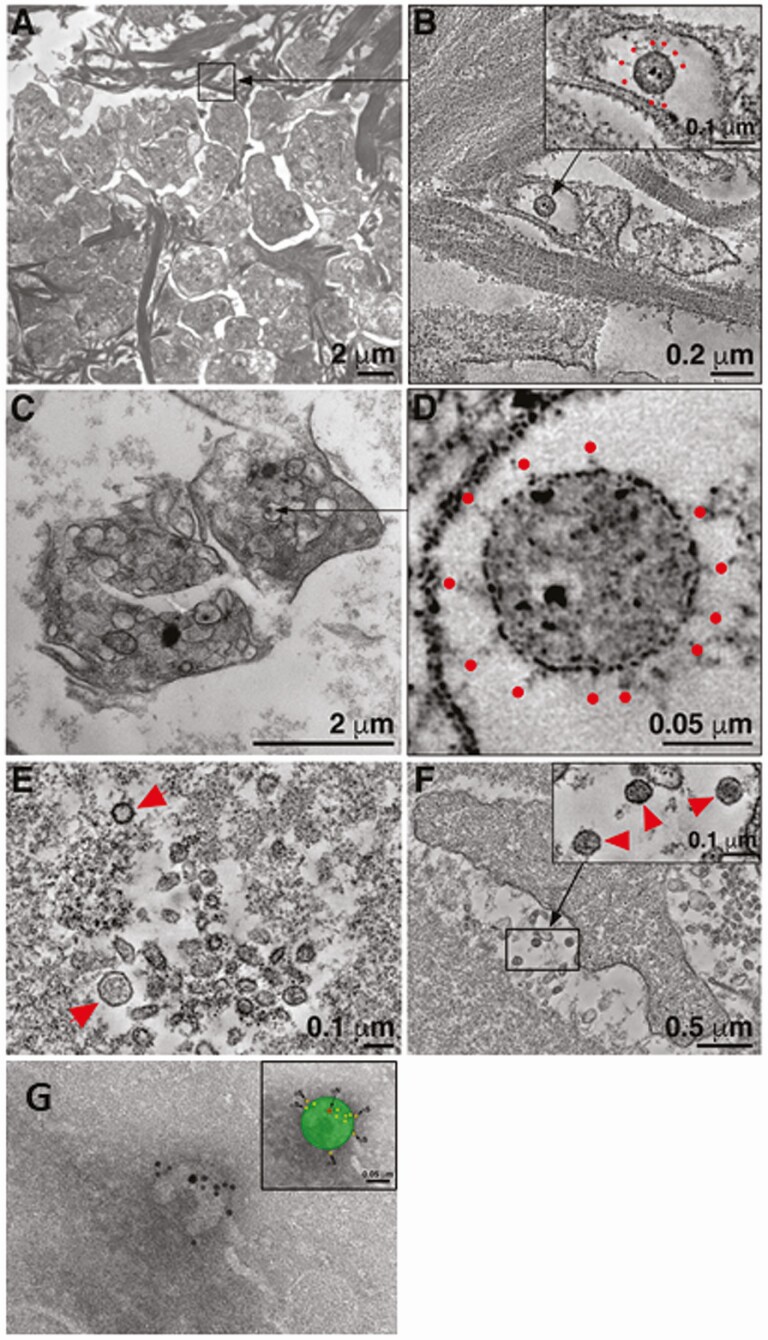
Methods: SARS-CoV-2 vRNA was quantified in plasma samples from observational cohorts of 51 COVID-19 patients including 9 outpatients, 19 hospitalized (non-intensive care unit [ICU]), and 23 ICU patients. vRNA levels were compared with cross-sectional indices of COVID-19 severity and prospective clinical outcomes. We used multiple imaging methods to visualize virions in plasma.
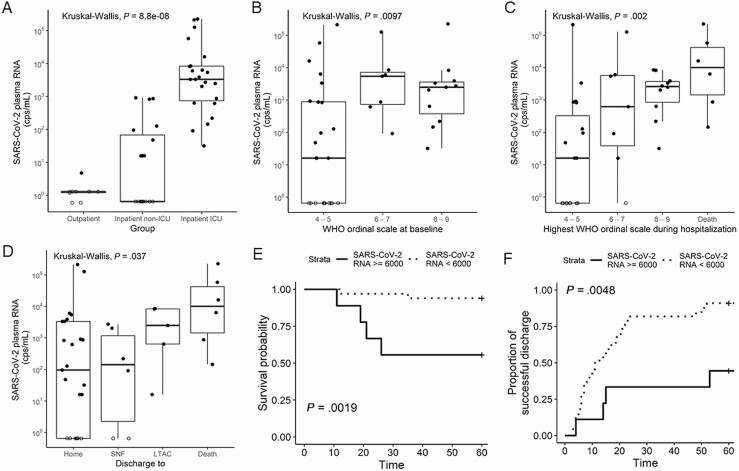
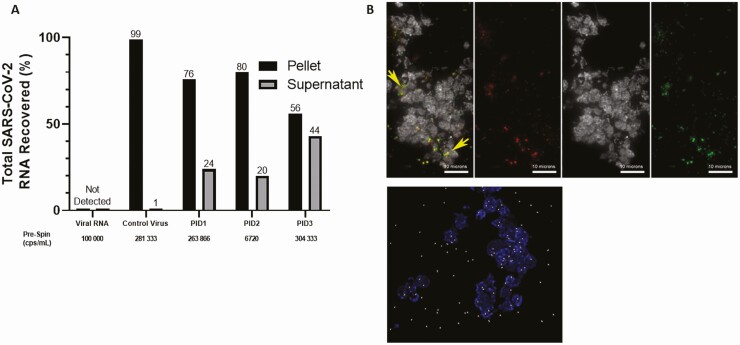
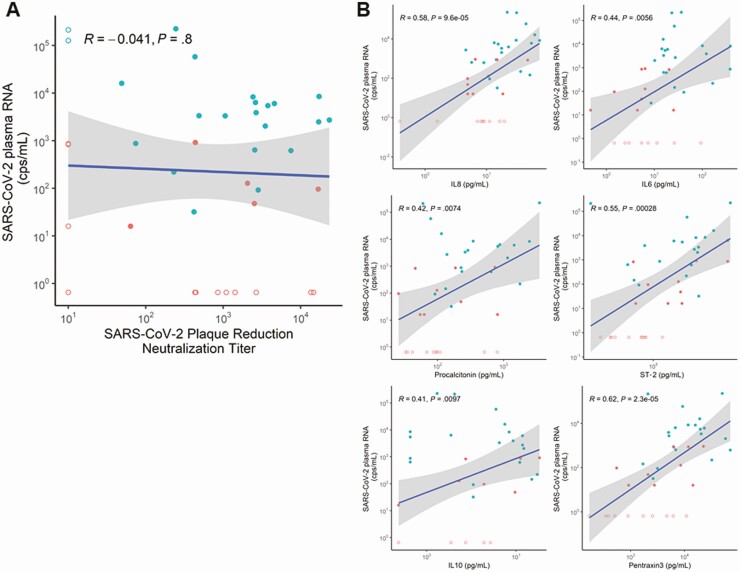
Results: SARS-CoV-2 vRNA was detected in plasma of 100%, 52.6%, and 11.1% of ICU, non-ICU, and outpatients, respectively. Virions were detected in plasma pellets using electron tomography and immunostaining. Plasma vRNA levels were significantly higher in ICU > non-ICU > outpatients (P < .0001); for inpatients, plasma vRNA levels were strongly associated with higher World Health Organization (WHO) score at admission (P = .01), maximum WHO score (P = .002), and discharge disposition (P = .004). A plasma vRNA level >6000 copies/mL was strongly associated with mortality (hazard ratio, 10.7). Levels of vRNA were significantly associated with several inflammatory biomarkers (P < .01) but not with plasma neutralizing antibody titers (P = .8).
Conclusions: Visualization of virus particles in plasma indicates that SARS-CoV-2 RNAemia is due, at least in part, to viremia. The levels of SARS-CoV-2 RNAemia correlate strongly with disease severity, patient outcome, and specific inflammatory biomarkers but not with neutralizing antibody titers.
Keywords: 19 outcome; 2 RNAemia; 2 viremia; COVID; CoV; SARS.
© The Author(s) 2021. Published by Oxford University Press for the Infectious Diseases Society of America. All rights reserved. For permissions, e-mail: journals.permissions@oup.com.
Figures
References
-
- Wiersinga WJ, Rhodes A, Cheng AC, Peacock SJ, Prescott HC. Pathophysiology, transmission, diagnosis, and treatment of coronavirus disease 2019 (COVID-19): a review. JAMA 2020; 324:782-93. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
