

Host lipidome and tuberculosis treatment failure
- PMID: 34375300
- PMCID: PMC9625841
- DOI: 10.1183/13993003.04532-2020
Host lipidome and tuberculosis treatment failure
Abstract
Introduction: Host lipids play important roles in tuberculosis (TB) pathogenesis. Whether host lipids at TB treatment initiation (baseline) affect subsequent treatment outcomes has not been well characterised. We used unbiased lipidomics to study the prospective association of host lipids with TB treatment failure.
Methods: A case-control study (n=192), nested within a prospective cohort study, was used to investigate the association of baseline plasma lipids with TB treatment failure among adults with pulmonary TB. Cases (n=46) were defined as TB treatment failure, while controls (n=146) were those without failure. Complex lipids and inflammatory lipid mediators were measured using liquid chromatography mass spectrometry techniques. Adjusted least-square regression was used to assess differences in groups. In addition, machine learning identified lipids with highest area under the curve (AUC) to classify cases and controls.
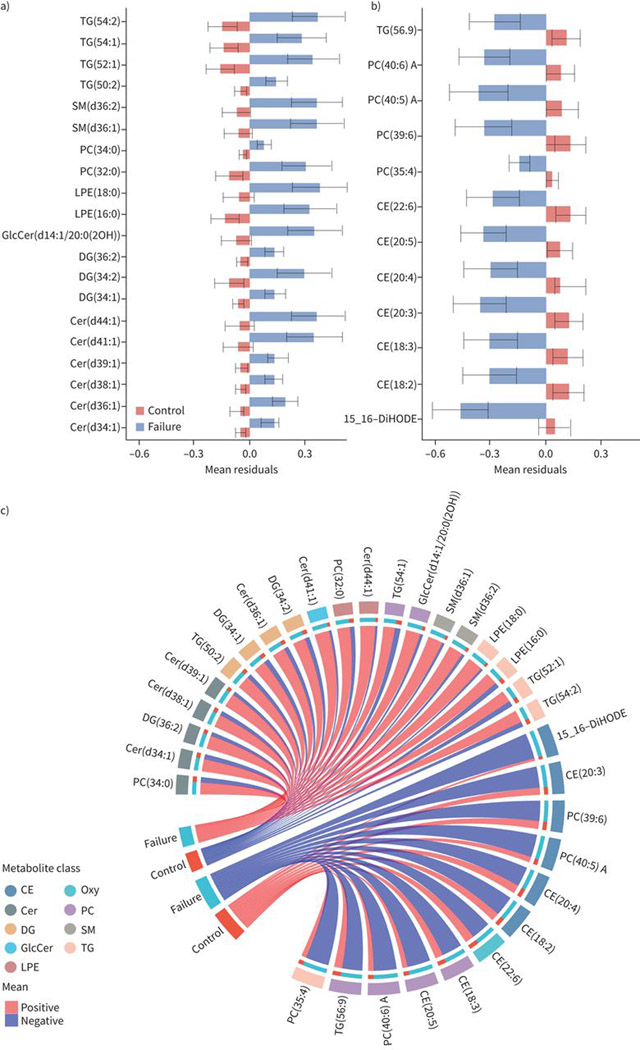
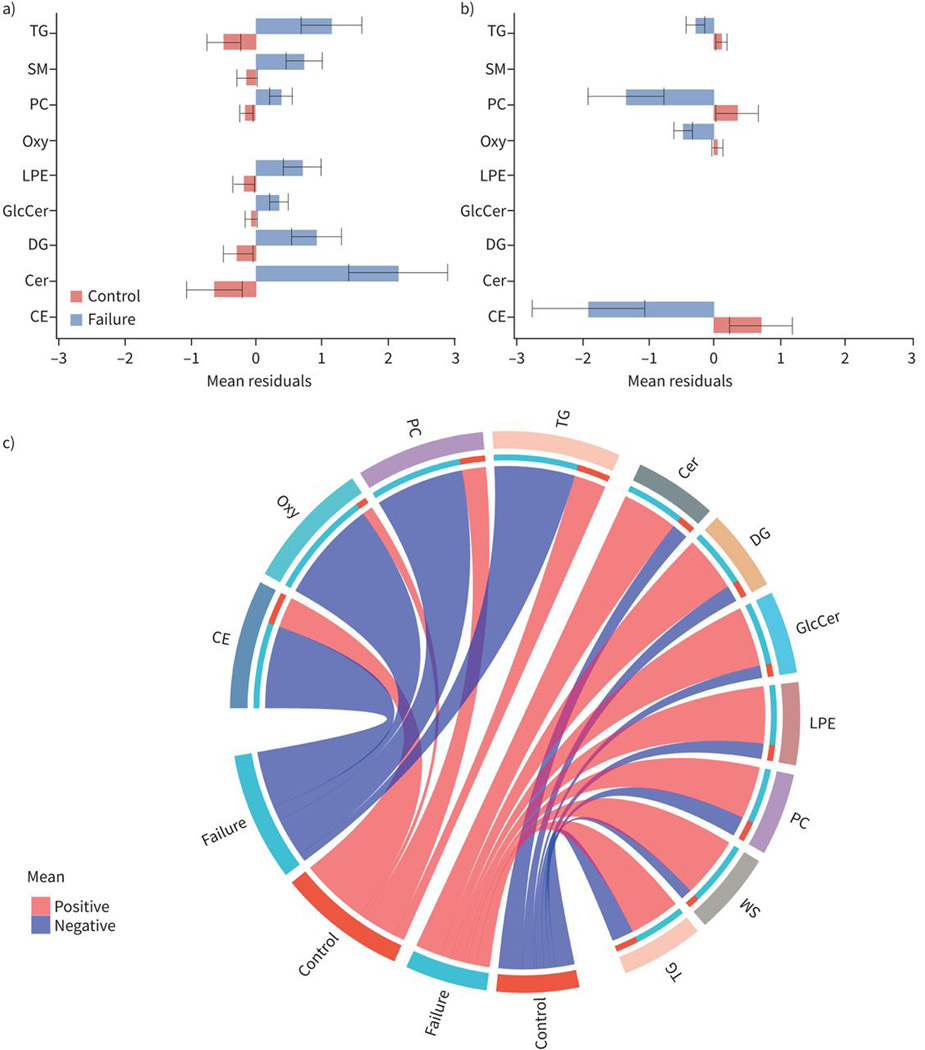
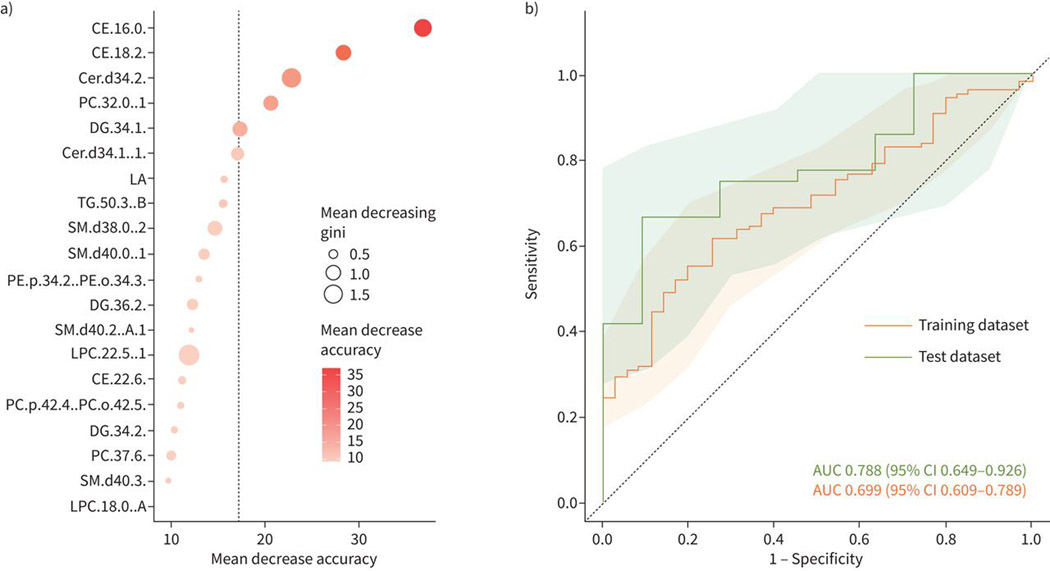
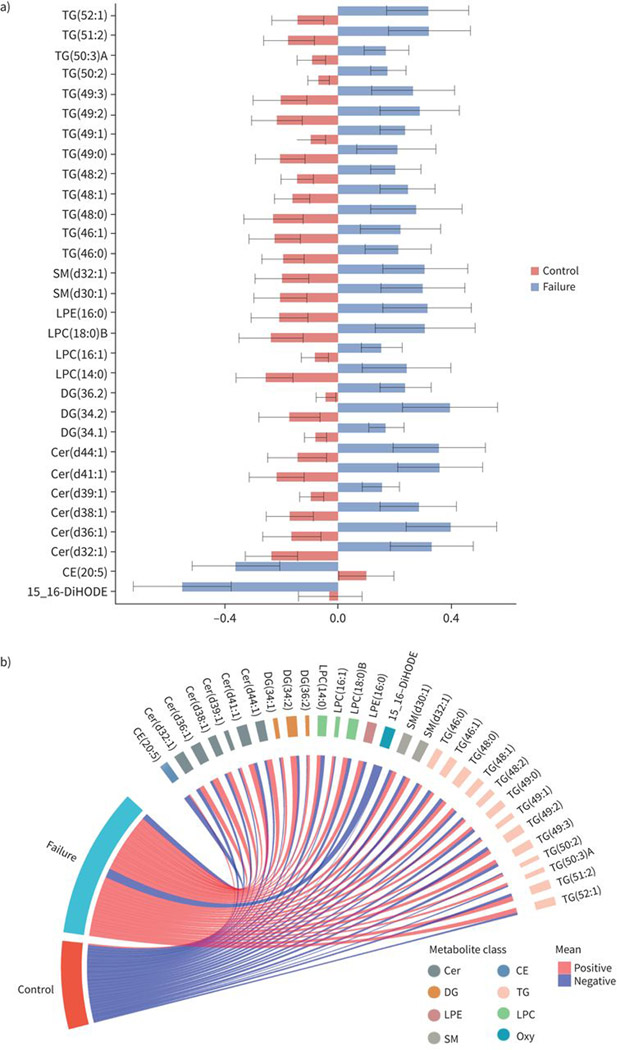
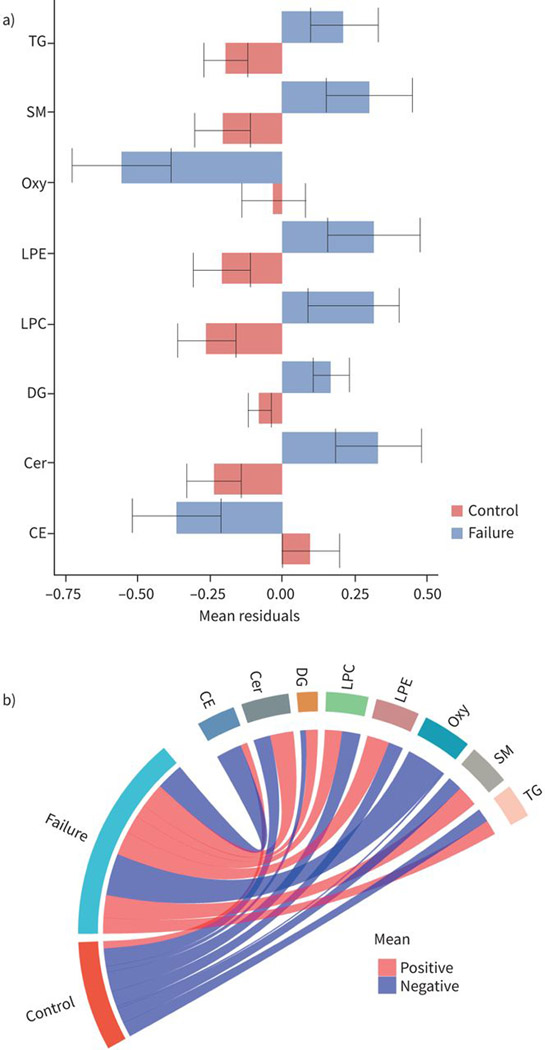
Results: Baseline levels of 32 lipids differed between controls and those with treatment failure after false discovery rate adjustment. Treatment failure was associated with lower baseline levels of cholesteryl esters and oxylipin, and higher baseline levels of ceramides and triglycerides compared to controls. Two cholesteryl ester lipids combined in a unique classifier model provided an AUC of 0.79 (95% CI 0.65-0.93) in the test dataset for prediction of TB treatment failure.
Conclusions: We identified lipids, some with known roles in TB pathogenesis, associated with TB treatment failure. In addition, a lipid signature with prognostic accuracy for TB treatment failure was identified. These lipids could be potential targets for risk-stratification, adjunct therapy and treatment monitoring.
Copyright ©The authors 2022. For reproduction rights and permissions contact permissions@ersnet.org.
Conflict of interest statement
Conflict of interest: R. Shivakoti reports grants from NIH, during the conduct of the study. Conflict of interest: J.W. Newman has nothing to disclose. Conflict of interest: L.E. Hanna has nothing to disclose. Conflict of interest: A.T.L. Queiroz has nothing to disclose. Conflict of interest: K. Borkowski has nothing to disclose. Conflict of interest: A.N. Gupte has nothing to disclose. Conflict of interest: M. Paradkar has nothing to disclose. Conflict of interest: P. Satyamurthi has nothing to disclose. Conflict of interest: V. Kulkarni has nothing to disclose. Conflict of interest: M. Selva has nothing to disclose. Conflict of interest: N. Pradhan has nothing to disclose. Conflict of interest: S.V.B.Y. Shivakumar has nothing to disclose. Conflict of interest: S. Natarajan has nothing to disclose. Conflict of interest: R. Karunaianantham has nothing to disclose. Conflict of interest: N. Gupte has nothing to disclose. Conflict of interest: K. Thiruvengadam has nothing to disclose. Conflict of interest: O. Fiehn has nothing to disclose. Conflict of interest: R. Bharadwaj has nothing to disclose. Conflict of interest: A. Kagal has nothing to disclose. Conflict of interest: S. Gaikwad has nothing to disclose. Conflict of interest: S. Sangle has nothing to disclose. Conflict of interest: J.E. Golub has nothing to disclose. Conflict of interest: B.B. Andrade has nothing to disclose. Conflict of interest: V. Mave reports grants from NIH, during the conduct of the study. Conflict of interest: A. Gupta reports grants from NIH, during the conduct of the study. Conflict of interest: C. Padmapriyadarsini has nothing to disclose.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical