

Effect of electroencephalography-guided anesthesia on neurocognitive disorders in elderly patients undergoing major non-cardiac surgery: A trial protocol The POEGEA trial (POncd Elderly GEneral Anesthesia)
- PMID: 34375362
- PMCID: PMC8354438
- DOI: 10.1371/journal.pone.0255852
Effect of electroencephalography-guided anesthesia on neurocognitive disorders in elderly patients undergoing major non-cardiac surgery: A trial protocol The POEGEA trial (POncd Elderly GEneral Anesthesia)
Abstract
Introduction: The number of elderly patients undergoing major surgery is rapidly increasing. They are particularly at risk of developing postoperative neurocognitive disorders (NCD). Earlier studies suggested that processed electroencephalographic (EEG) monitors may reduce the incidence of postoperative NCD. However, none of these studies controlled for intraoperative nociception levels or personalized blood pressure targets. Their results remain unclear if the reduction in the incidence of postoperative NCD relates to avoidance of any electroencephalographic pattern suggesting excessive anesthesia depth.
Objective: The objective of this trial is to investigate-in patients ≥ 70 years old undergoing major non-cardiac surgery-the effect of EEG-guided anesthesia on postoperative NCD while controlling for intraoperative nociception, personalized blood pressure targets, and using detailed information provided by the EEG monitor (including burst suppression ratio, density spectral array, and raw EEG waveform).
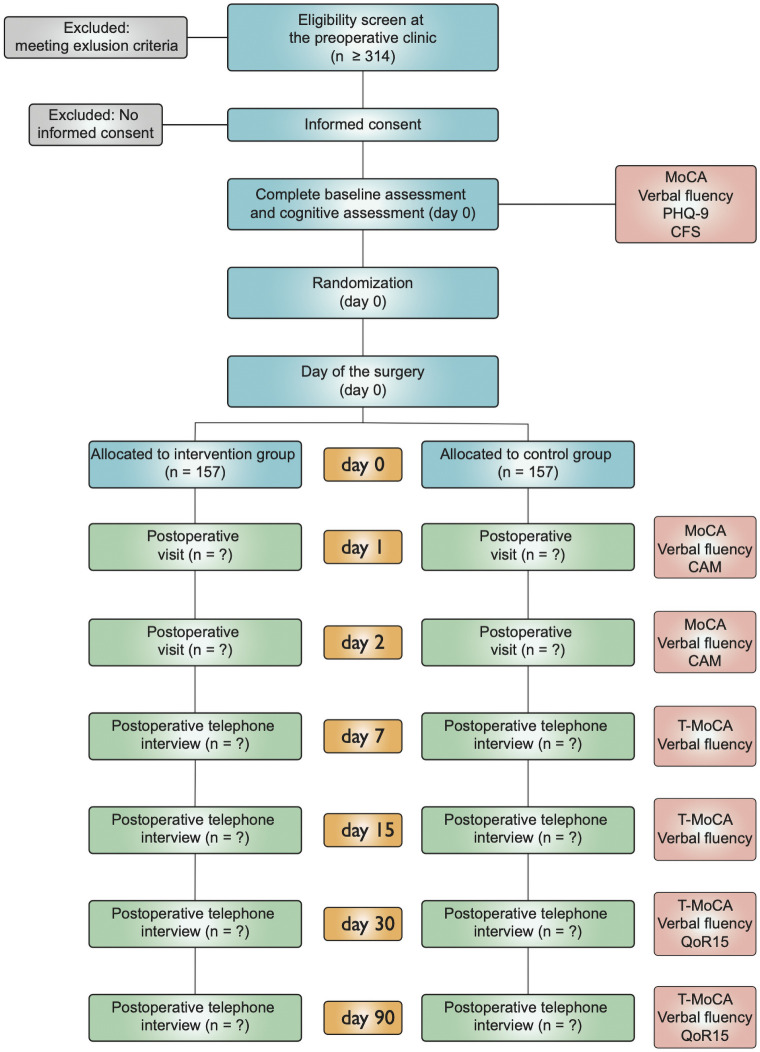
Material and methods: This prospective, randomized, controlled trial will be conducted in a single Canadian university hospital. Patients ≥ 70 years old undergoing elective major non-cardiac surgery will be included in the trial. The administration of sevoflurane will be adjusted to maintain a BIS index value between 40 and 60, to keep a Suppression Ratio (SR) at 0%, to keep a direct EEG display without any suppression time and a spectrogram with most of the EEG wave frequency within the alpha, theta, and delta frequencies in the EEG-guided group. In the control group, sevoflurane will be administered to achieve an age-adjusted minimum alveolar concentration of [0.8-1.2]. In both groups, a nociception monitor will guide intraoperative opioid administration, individual blood pressure targets will be used, and cerebral oximetry used to tailor intraoperative hemodynamic management. The primary endpoint will be the incidence of NCD at postoperative day 1, as evaluated by the Montreal Cognitive Assessment (MoCA). Secondary endpoints will include the incidence of postoperative NCD at different time points and the evaluation of cognitive trajectories up to 90 days after surgery among EEG-guided and control groups.
Study registration: NCT04825847 on ClinicalTrials.gov.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Aubé DS, K. Le vieillissement au Québec: Institut national de santé publique du Québec; 2016. https://www.inspq.qc.ca/le-vieillissement-au-quebec.
-
- Indicateurs de santé 2011: Institut canadien d’information sur la santé (ICIS); 2011. https://secure.cihi.ca/free_products/health_indicators_2011_fr.pdf.
-
- Ballard C, Jones E, Gauge N, Aarsland D, Nilsen OB, Saxby BK, et al.. Optimised anaesthesia to reduce post operative cognitive decline (POCD) in older patients undergoing elective surgery, a randomised controlled trial. PLoS One. 2012;7(6):e37410. doi: 10.1371/journal.pone.0037410 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
