

Effect of Intravenous Fluid Treatment With a Balanced Solution vs 0.9% Saline Solution on Mortality in Critically Ill Patients: The BaSICS Randomized Clinical Trial
- PMID: 34375394
- PMCID: PMC8356144
- DOI: 10.1001/jama.2021.11684
Effect of Intravenous Fluid Treatment With a Balanced Solution vs 0.9% Saline Solution on Mortality in Critically Ill Patients: The BaSICS Randomized Clinical Trial
Abstract
Importance: Intravenous fluids are used for almost all intensive care unit (ICU) patients. Clinical and laboratory studies have questioned whether specific fluid types result in improved outcomes, including mortality and acute kidney injury.
Objective: To determine the effect of a balanced solution vs saline solution (0.9% sodium chloride) on 90-day survival in critically ill patients.
Design, setting, and participants: Double-blind, factorial, randomized clinical trial conducted at 75 ICUs in Brazil. Patients who were admitted to the ICU with at least 1 risk factor for worse outcomes, who required at least 1 fluid expansion, and who were expected to remain in the ICU for more than 24 hours were randomized between May 29, 2017, and March 2, 2020; follow-up concluded on October 29, 2020. Patients were randomized to 2 different fluid types (a balanced solution vs saline solution reported in this article) and 2 different infusion rates (reported separately).
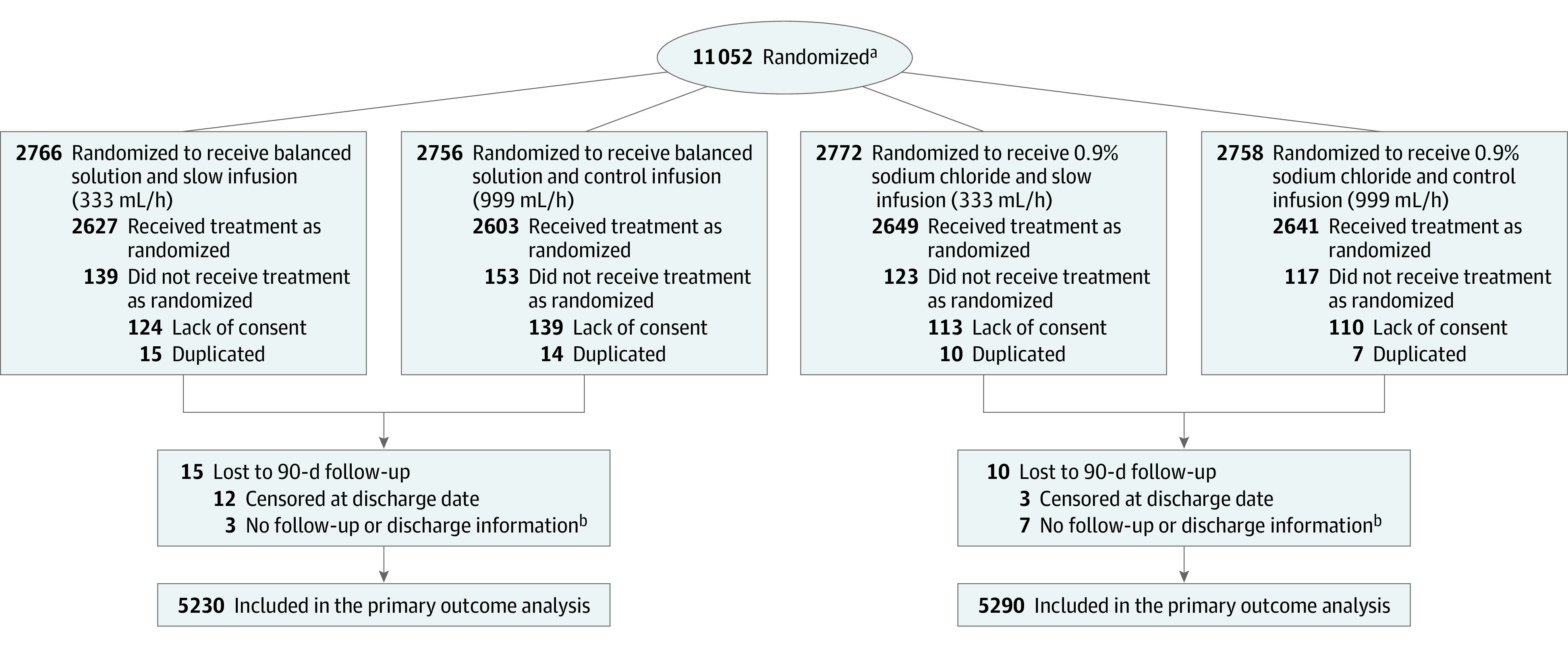
Interventions: Patients were randomly assigned 1:1 to receive either a balanced solution (n = 5522) or 0.9% saline solution (n = 5530) for all intravenous fluids.
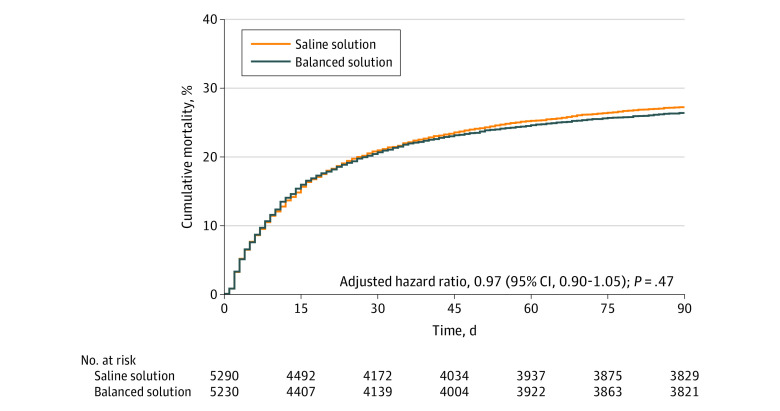
Main outcomes and measures: The primary outcome was 90-day survival.
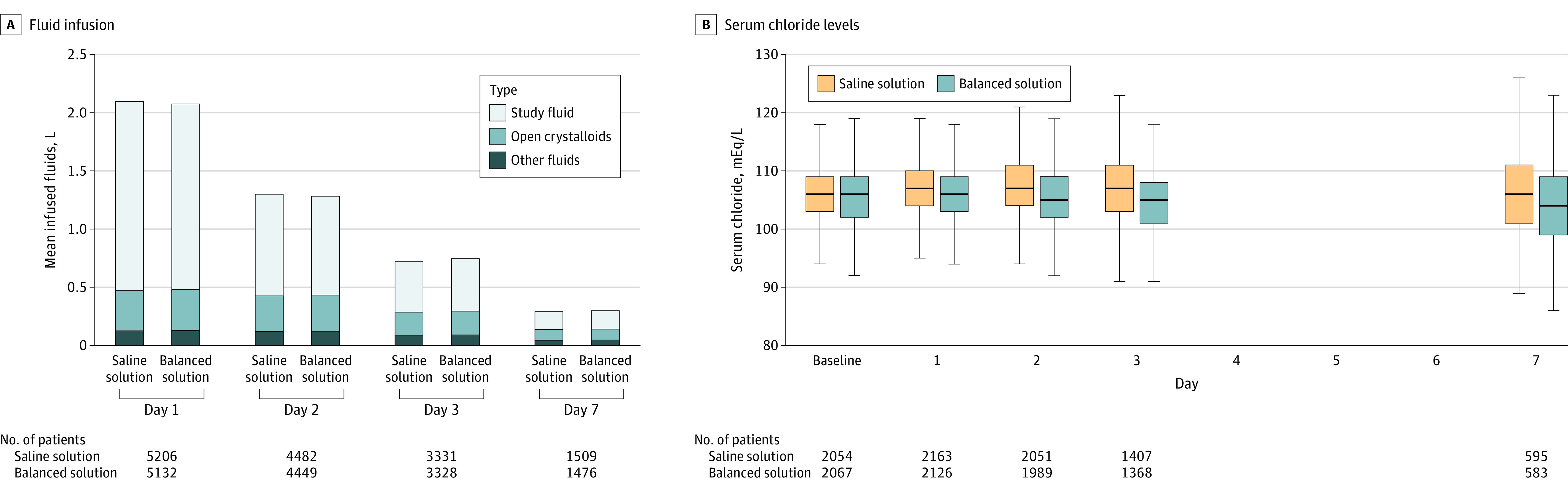
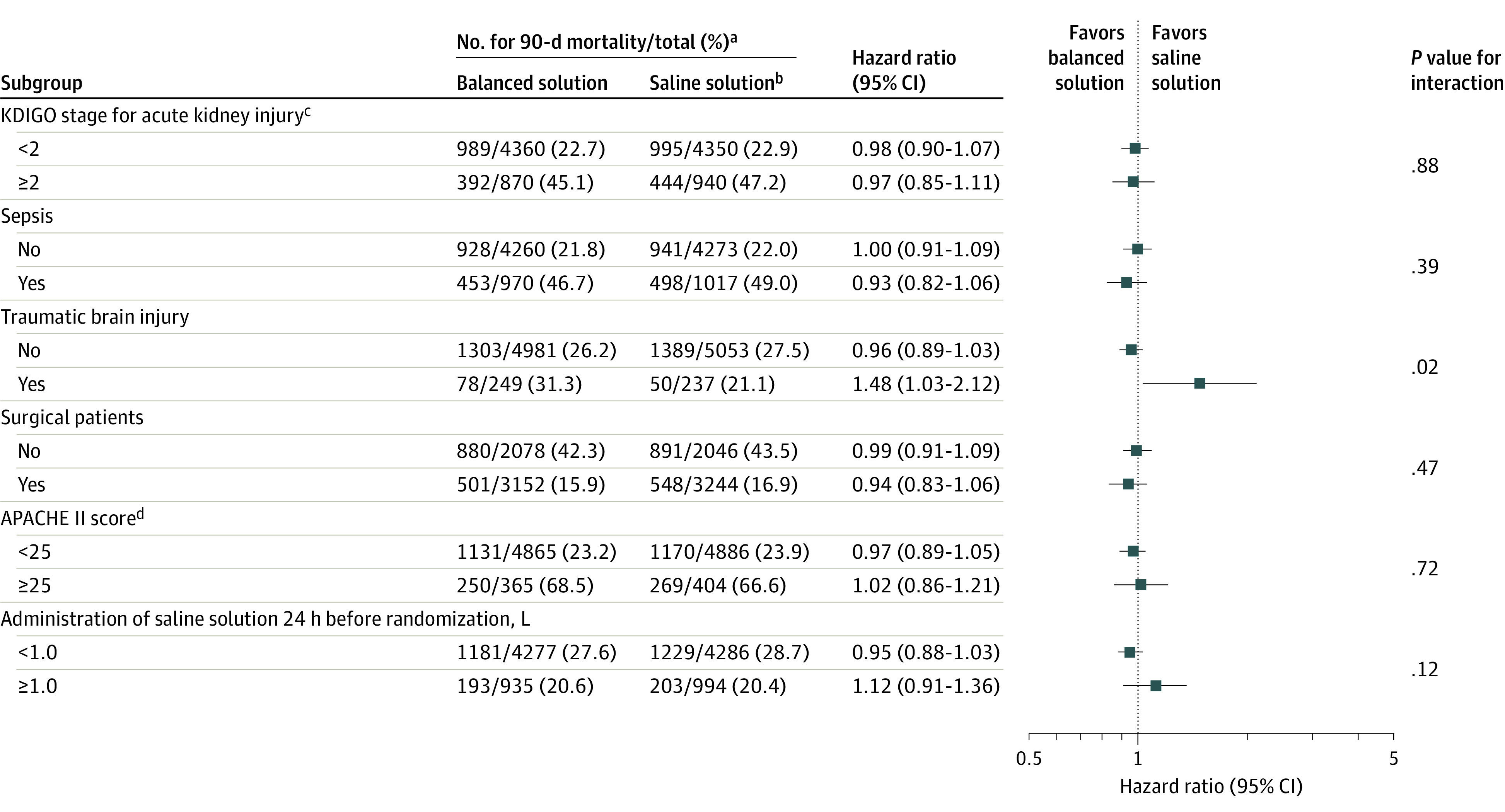
Results: Among 11 052 patients who were randomized, 10 520 (95.2%) were available for the analysis (mean age, 61.1 [SD, 17] years; 44.2% were women). There was no significant interaction between the 2 interventions (fluid type and infusion speed; P = .98). Planned surgical admissions represented 48.4% of all patients. Of all the patients, 60.6% had hypotension or vasopressor use and 44.3% required mechanical ventilation at enrollment. Patients in both groups received a median of 1.5 L of fluid during the first day after enrollment. By day 90, 1381 of 5230 patients (26.4%) assigned to a balanced solution died vs 1439 of 5290 patients (27.2%) assigned to saline solution (adjusted hazard ratio, 0.97 [95% CI, 0.90-1.05]; P = .47). There were no unexpected treatment-related severe adverse events in either group.
Conclusion and relevance: Among critically ill patients requiring fluid challenges, use of a balanced solution compared with 0.9% saline solution did not significantly reduce 90-day mortality. The findings do not support the use of this balanced solution.
Trial registration: ClinicalTrials.gov Identifier: NCT02875873.
Conflict of interest statement
Figures
Comment in
References
-
- Finfer S, Myburgh J, Bellomo R. Intravenous fluid therapy in critically ill adults. Published correction appears in Nat Rev Nephrol. 2018;14(11):717. Nat Rev Nephrol. 2018;14(9):541-557. - PubMed
-
- Yunos NM, Bellomo R, Hegarty C, et al. Association between a chloride-liberal vs chloride-restrictive intravenous fluid administration strategy and kidney injury in critically ill adults. JAMA. 2012;308(15):1566-1572. - PubMed
-
- Raghunathan K, Shaw A, Nathanson B, et al. Association between the choice of IV crystalloid and in-hospital mortality among critically ill adults with sepsis. Crit Care Med. 2014;42(7):1585-1591. - PubMed
-
- Zampieri FG, Ranzani OT, Azevedo LC, et al. Lactated ringer is associated with reduced mortality and less acute kidney injury in critically ill patients: a retrospective cohort analysis. Crit Care Med. 2016;44(12):2163-2170. - PubMed
Associated data
LinkOut - more resources
Full Text Sources
Medical
