

Machine learning model for early prediction of acute kidney injury (AKI) in pediatric critical care
- PMID: 34376222
- PMCID: PMC8353807
- DOI: 10.1186/s13054-021-03724-0
Machine learning model for early prediction of acute kidney injury (AKI) in pediatric critical care
Abstract
Background: Acute kidney injury (AKI) in pediatric critical care patients is diagnosed using elevated serum creatinine, which occurs only after kidney impairment. There are no treatments other than supportive care for AKI once it has developed, so it is important to identify patients at risk to prevent injury. This study develops a machine learning model to learn pre-disease patterns of physiological measurements and predict pediatric AKI up to 48 h earlier than the currently established diagnostic guidelines.
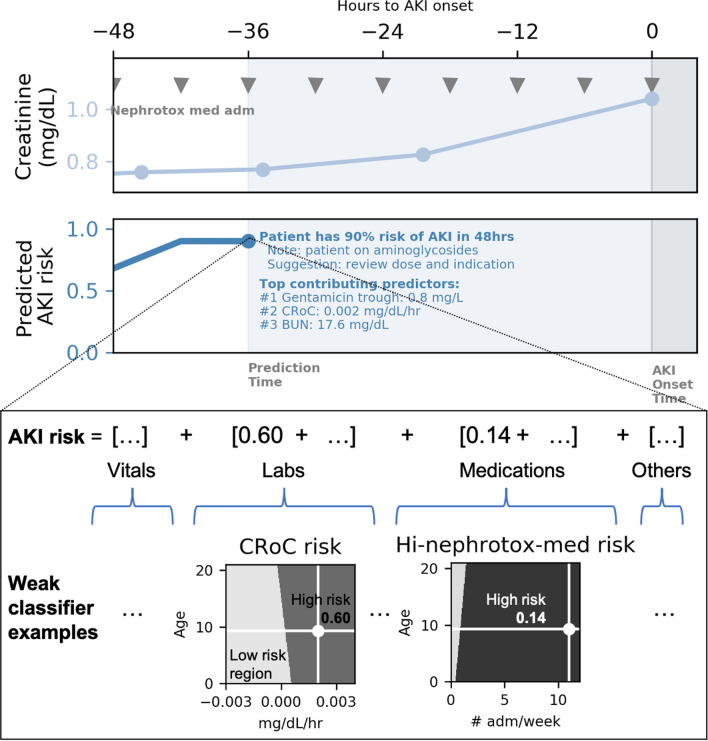
Methods: EHR data from 16,863 pediatric critical care patients between 1 month to 21 years of age from three independent institutions were used to develop a single machine learning model for early prediction of creatinine-based AKI using intelligently engineered predictors, such as creatinine rate of change, to automatically assess real-time AKI risk. The primary outcome is prediction of moderate to severe AKI (Stage 2/3), and secondary outcomes are prediction of any AKI (Stage 1/2/3) and requirement of renal replacement therapy (RRT). Predictions generate alerts allowing fast assessment and reduction of AKI risk, such as: "patient has 90% risk of developing AKI in the next 48 h" along with contextual information and suggested response such as "patient on aminoglycosides, suggest check level and review dose and indication".
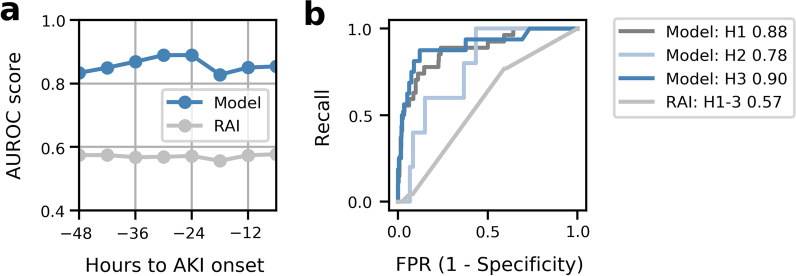
Results: The model was successful in predicting Stage 2/3 AKI prior to detection by conventional criteria with a median lead-time of 30 h at AUROC of 0.89. The model predicted 70% of subsequent RRT episodes, 58% of Stage 2/3 episodes, and 41% of any AKI episodes. The ratio of false to true alerts of any AKI episodes was approximately one-to-one (PPV 47%). Among patients predicted, 79% received potentially nephrotoxic medication after being identified by the model but before development of AKI.
Conclusions: As the first multi-center validated AKI prediction model for all pediatric critical care patients, the machine learning model described in this study accurately predicts moderate to severe AKI up to 48 h in advance of AKI onset. The model may improve outcome of pediatric AKI by providing early alerting and actionable feedback, potentially preventing or reducing AKI by implementing early measures such as medication adjustment.
Keywords: AKI; Acute kidney injury; Machine learning; Pediatric critical care; Predictive model.
© 2021. The Author(s).
Conflict of interest statement
CN serves as consultant to Philips Research.
Figures
References
-
- Kellum JA, Lameire N, Aspelin P, Barsoum RS, Burdmann EA, Goldstein SL, Herzog CA, Joannidis M, Kribben A, Levey AS, MacLeod AM. Kidney disease: improving global outcomes (KDIGO) acute kidney injury work group. KDIGO clinical practice guideline for acute kidney injury. Kidney Int Suppl. 2012;2(1):1–138. doi: 10.1038/kisup.2012.1. - DOI
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
