

Oncogene-specific differences in tumor mutational burden, PD-L1 expression, and outcomes from immunotherapy in non-small cell lung cancer
- PMID: 34376553
- PMCID: PMC8356172
- DOI: 10.1136/jitc-2021-002891
Oncogene-specific differences in tumor mutational burden, PD-L1 expression, and outcomes from immunotherapy in non-small cell lung cancer
Abstract
Background: Non-small cell lung cancer (NSCLC) patients bearing targetable oncogene alterations typically derive limited benefit from immune checkpoint blockade (ICB), which has been attributed to low tumor mutation burden (TMB) and/or PD-L1 levels. We investigated oncogene-specific differences in these markers and clinical outcome.
Methods: Three cohorts of NSCLC patients with oncogene alterations (n=4189 total) were analyzed. Two clinical cohorts of advanced NSCLC patients treated with ICB monotherapy [MD Anderson (MDACC; n=172) and Flatiron Health-Foundation Medicine Clinico-Genomic Database (CGDB; n=894 patients)] were analyzed for clinical outcome. The FMI biomarker cohort (n=4017) was used to assess the association of oncogene alterations with TMB and PD-L1 expression.
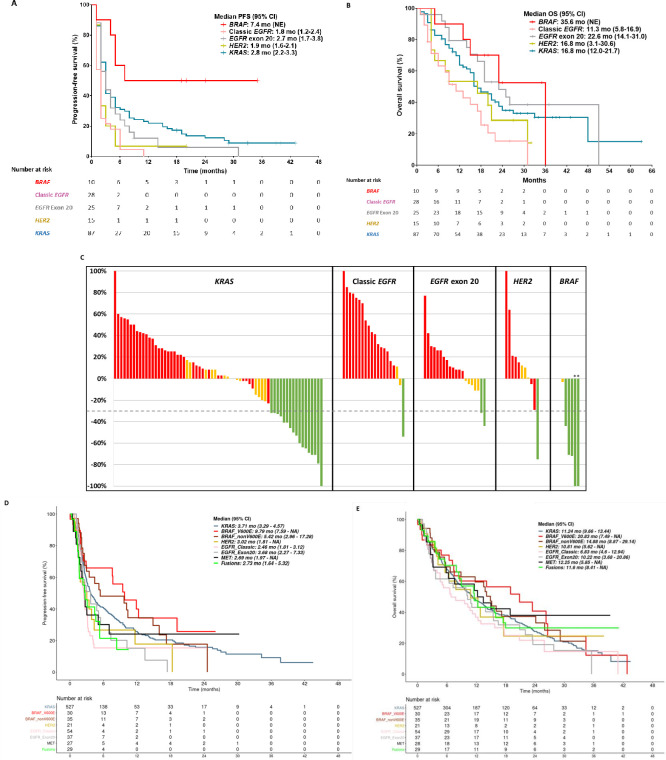
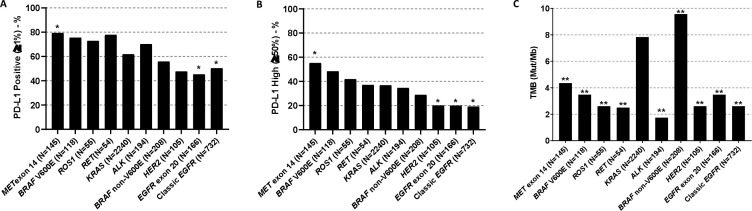
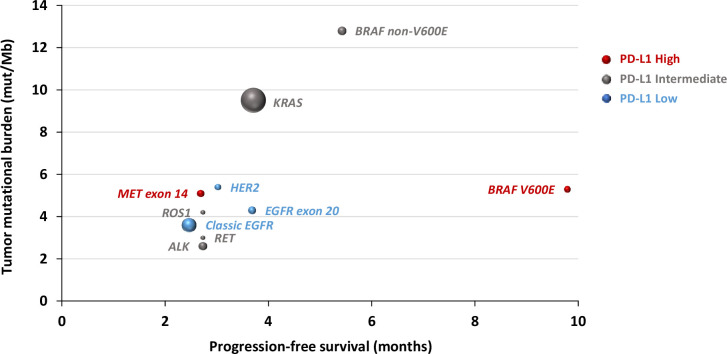
Results: High PD-L1 expression (PD-L1 ≥50%) rate was 19%-20% in classic EGFR, EGFR exon 20 and HER2-mutant tumors, and 34%-55% in tumors with ALK, BRAF V600E, ROS1, RET, or MET alterations. Compared with KRAS-mutant tumors, BRAF non-V600E group had higher TMB (9.6 vs KRAS 7.8 mutations/Mb, p=0.003), while all other oncogene groups had lower TMB (p<0.001). In the two clinical cohorts treated with ICB, molecular groups with EGFR, HER2, ALK, ROS1, RET, or MET alterations had short progression-free survival (PFS; 1.8-3.7 months), while BRAF V600E group was associated with greater clinical benefit from ICB (CGDB cohort: PFS 9.8 months vs KRAS 3.7 months, HR 0.66, p=0.099; MDACC cohort: response rate 62% vs KRAS 24%; PFS 7.4 vs KRAS 2.8 months, HR 0.36, p=0.026). KRAS G12C and non-G12C subgroups had similar clinical benefit from ICB in both cohorts. In a multivariable analysis, BRAF V600E mutation (HR 0.58, p=0.041), PD-L1 expression (HR 0.57, p=0.022), and high TMB (HR 0.66, p<0.001) were associated with longer PFS.
Conclusions: High TMB and PD-L1 expression are predictive for benefit from ICB treatment in oncogene-driven NSCLCs. NSCLC harboring BRAF mutations demonstrated superior benefit from ICB that may be attributed to higher TMB and higher PD-L1 expression in these tumors. Meanwhile EGFR and HER2 mutations and ALK, ROS1, RET, and MET fusions define NSCLC subsets with minimal benefit from ICB despite high PD-L1 expression in NSCLC harboring oncogene fusions. These findings indicate a TMB/PD-L1-independent impact on sensitivity to ICB for certain oncogene alterations.
Keywords: immunotherapy; lung neoplasms; tumor biomarkers.
© Author(s) (or their employer(s)) 2021. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: MVN is a consultant for Mirati and Merck/MSD, and reports funding to the institution from Mirati, Novartis, Pfizer, Ziopharm, AstraZeneca, and Checkmate; MM is an employee of Foundation Medicine, and owns stock in Roche; KS is an employee of Genentech, and owns stock in Roche; IB is an employee of Genentech, owns stock in Roche; VS is an employee of Roche, and owns stock in Roche; HX is an employee of Roche, and owns stock in Roche; HS is an employee of Genentech, and owns stock in Roche; XL is a Consultant for Eli Lilly, AstraZeneca, and EMD Serono; MEG is a former employee of Foundation Medicine; KM is an employee of Foundation Medicine, and owns stock in Roche; JPR reports licensing/royalties from Spectrum Pharmaceuticals; TC has received speaker’s fees from the Society for Immunotherapy of Cancer and Bristol-Myers Squibb, receives consulting fees from MedImmune and Bristol-Myers Squibb, and reports research funding to MD Anderson Cancer Center from Boehringer Ingelheim, MedImmune and Bristol-Myers Squibb; AT reports research grants from Eli Lilly, Millennium, Polaris, Genentech, Merck, Boehringer-Ingelheim, BMS, Ariad, Epizyme, Seattle Genetics, Takeda, and EMD Serono; advisory board member for BMS, Eli Lilly, Genentech, Roche, Novartis, Ariad, EMD Serono, Merck, Seattle Genetics, Astra-Zeneca, Boehringer-Ingelheim, Sellas Life Science, Takeda, Epizyme, and Huron; VP is an employee of Pfizer; DLG reports research grants from AstraZeneca, Jenssen R & D, Takeda, Ribun Therapeutics; and honoraria member of Senofi, AstraZeneca, Ribun Therapeutics; GS is an employee of Foundation Medicine, and owns stock in Roche; VAM is an employee of Foundation Medicine, and owns stock in Roche; BA is an employee of Foundation Medicine, and owns stock in Roche; GF is an employee of Foundation Medicine, and owns stock in Roche; LAA is an employee of Foundation Medicine, and owns stock in Roche; DS is an employee of Genentech, and owns stock in Roche; JZ reports research funding from Merck, Johnson and Johnson, and consultant fees from BMS, Johnson and Johnson, AstraZeneca, Geneplus, OrigMed, Innovent outside the submitted work; JVH reports research grants from NIH/NCI, American Cancer Society, Cancer Prevention & Research Institute of Texas, AACR Johnson & Johnson Lung Cancer, AZ, Spectrum, Checkmate Pharmaceuticals; Advisory Committees – AZ, BMS, GSK, Guardant Health, Kairos Venture Investments, BrightPath Biotherapeutics Hengrui Therapeutics, Eli Lilly, Spectrum, EMD Serono, Roche, Foundation One Medicine; Royalties & Licensing – Spectrum & Bio-Tree Systems, Inc.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous