

Coronary In-Stent Restenosis: Predictors and Treatment
- PMID: 34379053
- PMCID: PMC8715314
- DOI: 10.3238/arztebl.m2021.0254
Coronary In-Stent Restenosis: Predictors and Treatment
Abstract
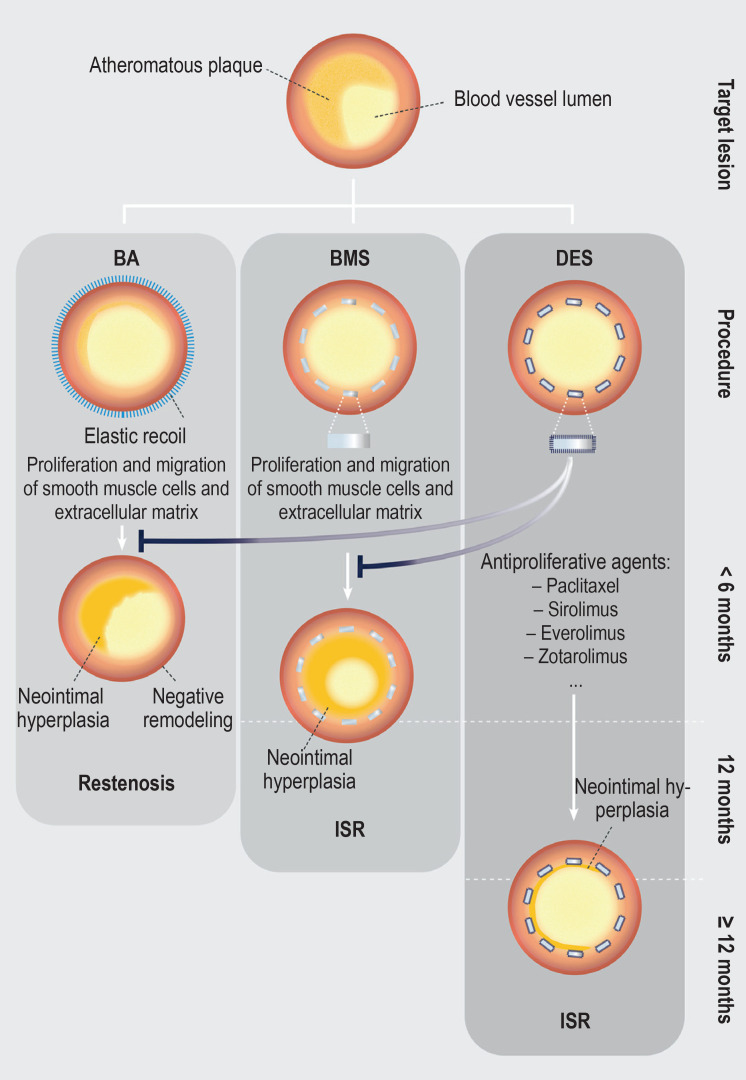
Background: Despite the use of modern drug-eluting stents (DES), in-stent restenosis (ISR) may still occur in as many as 2-10% of percutaneous coronary interventions (PCI) in certain lesion/patient subsets. ISR causes increased morbidity after stent implantation; acute myocardial infarction is a frequent correlate to a clinical ISR, arising in 5-10% of cases. Compared to de novo stenosis, patients with ISR also present more frequently with symptoms of unstable angina pectoris (45% versus 61%). In this article, we discuss the risk factors for ISR and the corresponding diagnostic measures and effective treatment strategies.
Methods: This review is based on pertinent publications retrieved by a selective search in PubMed, with special attention to current international guidelines and specialist society recommendations.
Results: The type of implanted stent, the presence of diabetes mellitus, previous bypass surgery, and small vessel caliber are predictors for ISR. In their guidelines, the European specialist societies (ESC/EACTS) recommend repeated PCI with DES implantation or drug-coated balloon (DCB) angioplasty as the methods of choice for the treatment of ISR. This approach is supported by evidence from meta-analyses. The RIBS-IV trial showed that revascularization treatment of the target lesion is needed less often after everolimus-eluting stent (EES) implantation than after DCB dilatation (11 [7.1%] versus 24 [15.6%]; p = 0.015; hazard ratio: 0.43; 95% confidence interval: [0.21; 0.87]).
Conclusion: Because the pathogenesis of ISR is multifactorial, differentiated risk stratification is necessary. The identification of patient-, stent-, and lesion-related predictors is particularly important, as the most effective way to combat ISR is to prevent it.
Figures
Comment in
-
Lipid Metabolism Disorders.Dtsch Arztebl Int. 2022 Apr 1;119(13):229. doi: 10.3238/arztebl.m2022.0057. Dtsch Arztebl Int. 2022. PMID: 35773985 Free PMC article. No abstract available.
-
In Reply.Dtsch Arztebl Int. 2022 Apr 1;119(13):229. doi: 10.3238/arztebl.m2022.0058. Dtsch Arztebl Int. 2022. PMID: 35773986 Free PMC article. No abstract available.
References
-
- Lee MS, Banka G. In-stent restenosis. Interv Cardiol Clin. 2016;5:211–220. - PubMed
-
- Stone GW, Ellis SG, Cox DA, et al. One-year clinical results with the slow-release, polymer-based, paclitaxel-eluting TAXUS stent: the TAXUS-IV trial. Circulation. 2004;109:1942–1947. - PubMed
-
- Kuntz RE, Baim DS. Defining coronary restenosis. Newer clinical and angiographic paradigms. Circulation. 1993;88:1310–1323. - PubMed
-
- Schühlen H, Kastrati A, Mehilli J, et al. Restenosis detected by routine angiographic follow-up and late mortality after coronary stent placement. Am Heart J. 2004;147:317–322. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous