

Genomic Autopsy of Sudden Deaths in Young Individuals
- PMID: 34379075
- PMCID: PMC8358810
- DOI: 10.1001/jamacardio.2021.2789
Genomic Autopsy of Sudden Deaths in Young Individuals
Abstract
Importance: Postmortem genetic testing of young individuals with sudden death has previously identified pathogenic gene variants. However, prior studies primarily considered highly penetrant monogenic variants, often without detailed decedent and family clinical information.
Objective: To assess genotype and phenotype risk in a diverse cohort of young decedents with sudden death and their families.
Design, setting, and participants: Pathological and whole-genome sequence analysis was conducted in a cohort referred from a national network of medical examiners. Cases were accrued prospectively from May 2015 to March 2019 across 24 US states. Analysis began September 2016 and ended November 2020.
Exposures: Evaluation of autopsy and clinical data integrated with whole-genome sequence data and family member evaluation.
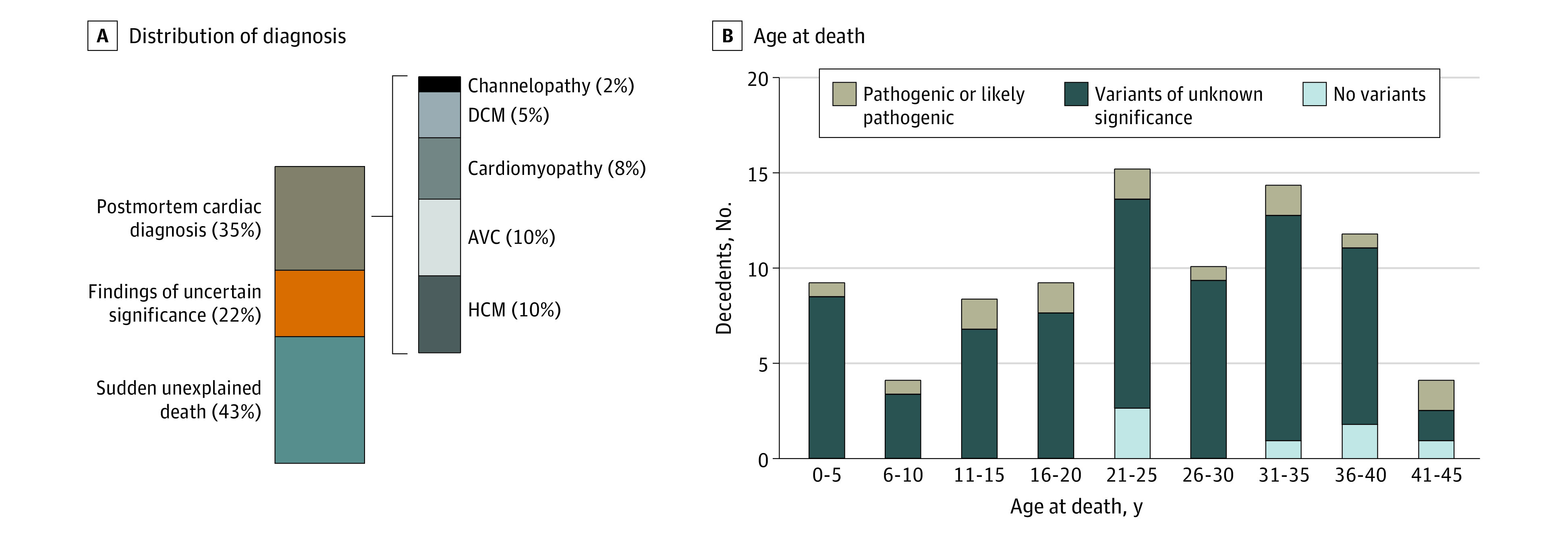
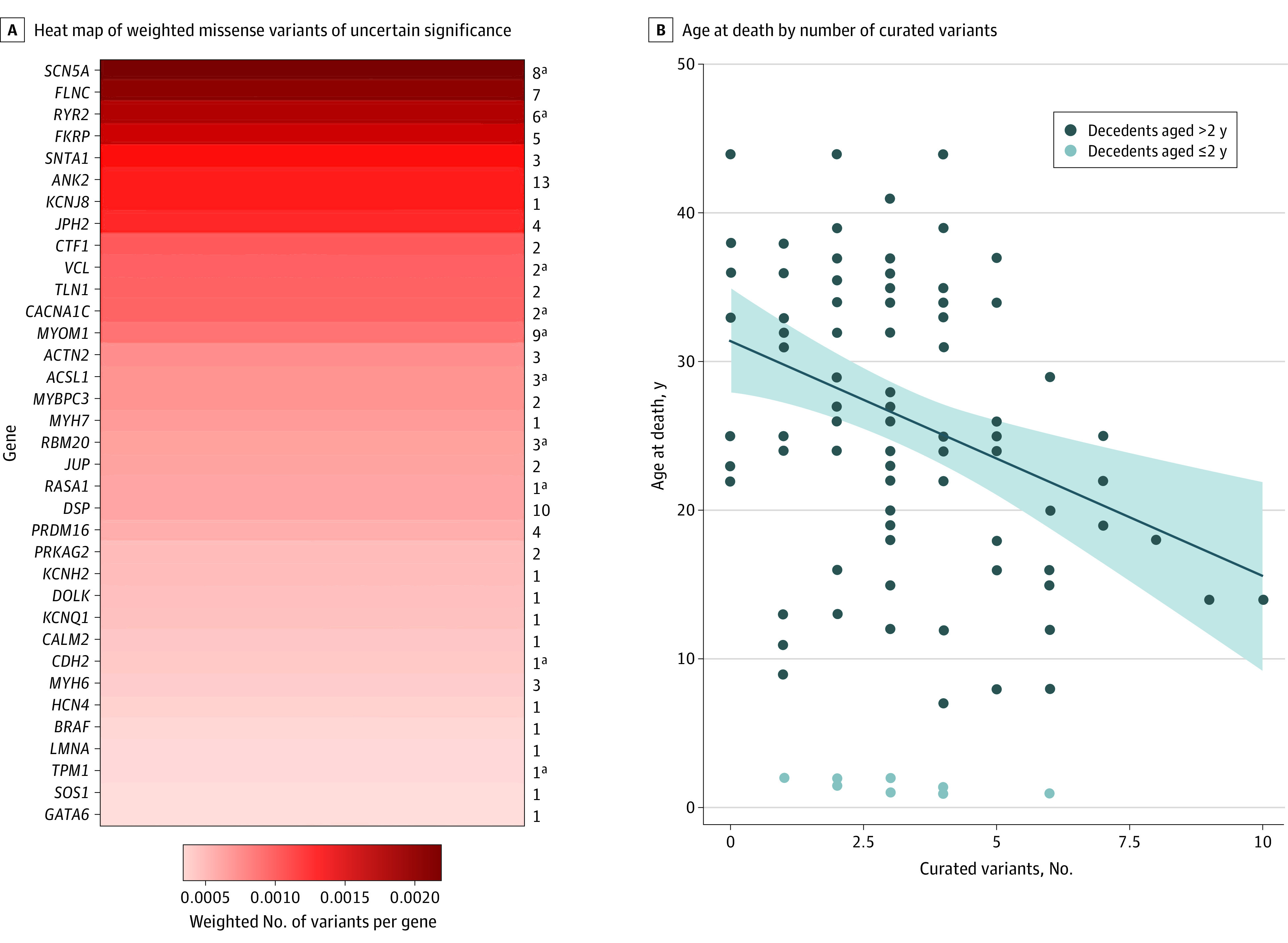
Results: A total of 103 decedents (mean [SD] age at death, 23.7 [11.9] years; age range, 1-44 years), their surviving family members, and 140 sex- and genetic ancestry-matched controls were analyzed. Among 103 decedents, autopsy and clinical data review categorized 36 decedents with postmortem diagnoses, 23 decedents with findings of uncertain significance, and 44 with sudden unexplained death. Pathogenic/likely pathogenic (P/LP) genetic variants in arrhythmia or cardiomyopathy genes were identified in 13 decedents (12.6%). A multivariable analysis including decedent phenotype, ancestry, and sex demonstrated that younger decedents had a higher burden of P/LP variants and select variants of uncertain significance (effect size, -1.64; P = .001). These select, curated variants of uncertain significance in cardiac genes were more common in decedents than controls (83 of 103 decedents [86%] vs 100 of 140 controls [71%]; P = .005), and decedents harbored more rare cardiac variants than controls (2.3 variants per individual vs 1.8 in controls; P = .006). Genetic testing of 31 parent-decedent trios and 14 parent-decedent dyads revealed 8 transmitted P/LP variants and 1 de novo P/LP variant. Incomplete penetrance was present in 6 of 8 parents who transmitted a P/LP variant.
Conclusions and relevance: Whole-genome sequencing effectively identified P/LP variants in cases of sudden death in young individuals, implicating both arrhythmia and cardiomyopathy genes. Genomic analyses and familial phenotype association suggest potentially additive, oligogenic risk mechanisms for sudden death in this cohort.
Conflict of interest statement
Figures
Comment in
-
Factors Affecting Yield of Genetic Testing of Sudden Deaths in Young Individuals-Reply.JAMA Cardiol. 2022 May 1;7(5):568-569. doi: 10.1001/jamacardio.2021.6026. JAMA Cardiol. 2022. PMID: 35195661 Free PMC article. No abstract available.
-
Factors Affecting Yield of Genetic Testing of Sudden Deaths in Young Individuals.JAMA Cardiol. 2022 May 1;7(5):568. doi: 10.1001/jamacardio.2021.6023. JAMA Cardiol. 2022. PMID: 35195662 Free PMC article. No abstract available.
References
-
- Mak CM, Mok NS, Shum HC, et al. Sudden arrhythmia death syndrome in young victims: a five-year retrospective review and two-year prospective molecular autopsy study by next-generation sequencing and clinical evaluation of their first-degree relatives. Hong Kong Med J. 2019;25(1):21-29. doi: 10.12809/hkmj187256 - DOI - PubMed
-
- Marcondes L, Crawford J, Earle N, et al. ; Cardiac Inherited Disease Group New Zealand . Long QT molecular autopsy in sudden unexplained death in the young (1-40 years old): lessons learnt from an eight year experience in New Zealand. PLoS One. 2018;13(4):e0196078. doi: 10.1371/journal.pone.0196078 - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
