

Assessment of Global Trends in the Diagnosis of Mesothelioma From 1990 to 2017
- PMID: 34379126
- PMCID: PMC8358735
- DOI: 10.1001/jamanetworkopen.2021.20360
Assessment of Global Trends in the Diagnosis of Mesothelioma From 1990 to 2017
Abstract
Importance: It is difficult for policy makers and clinicians to formulate targeted management strategies for mesothelioma because data on current epidemiological patterns worldwide are lacking.
Objective: To evaluate the mesothelioma burden across the world and describe its epidemiological distribution over time and by sociodemographic index (SDI) level, geographic location, sex, and age.
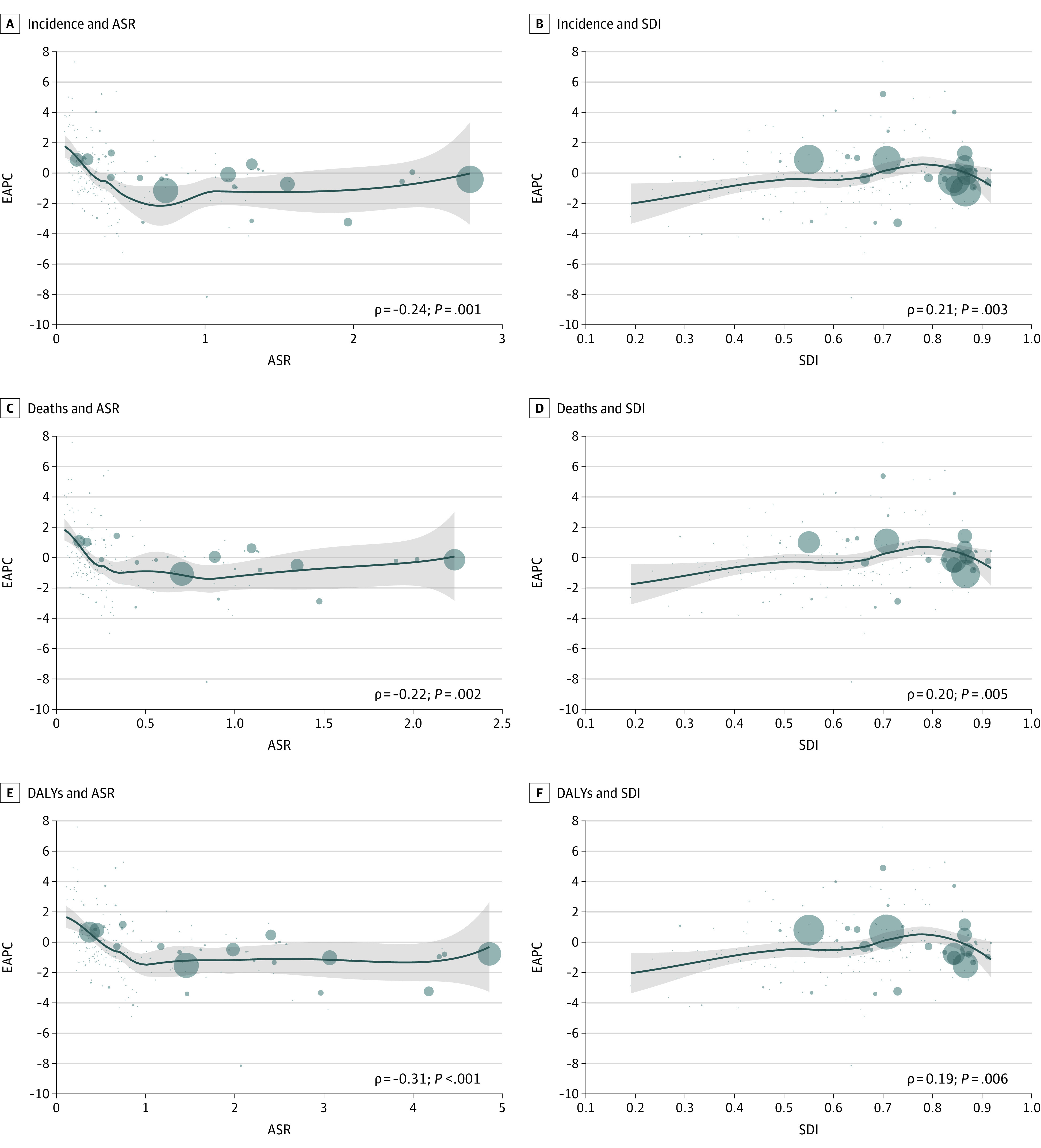
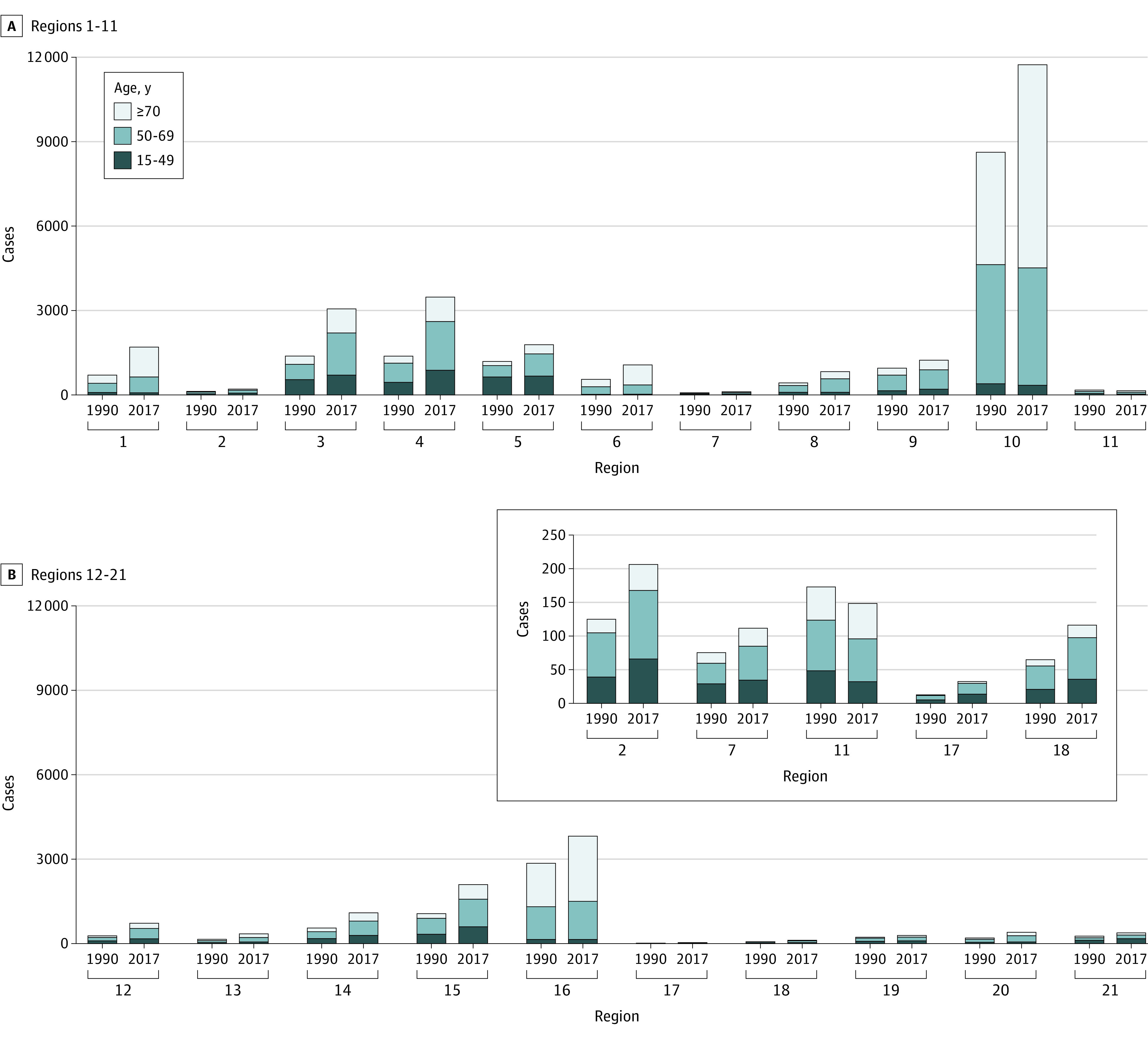
Design, setting, and participants: Annual case data and age-standardized rates of incidence, death, and disability-adjusted life-years associated with mesothelioma among different age groups were obtained from the Global Burden of Disease 2017 database. The estimated annual percentage changes in age-standardized rates were calculated to evaluate temporal trends in incidence and mortality. The study population comprised individuals from 21 regions in 195 countries and territories who were diagnosed with mesothelioma between 1990 and 2017. Data were collected from May 23, 2019, to January 18, 2020.
Main outcomes and measures: Primary outcomes were incident cases, deaths, and their age-standardized rates and estimated annual percentage changes. Secondary outcomes were disability-adjusted life-years and relative temporal trends.
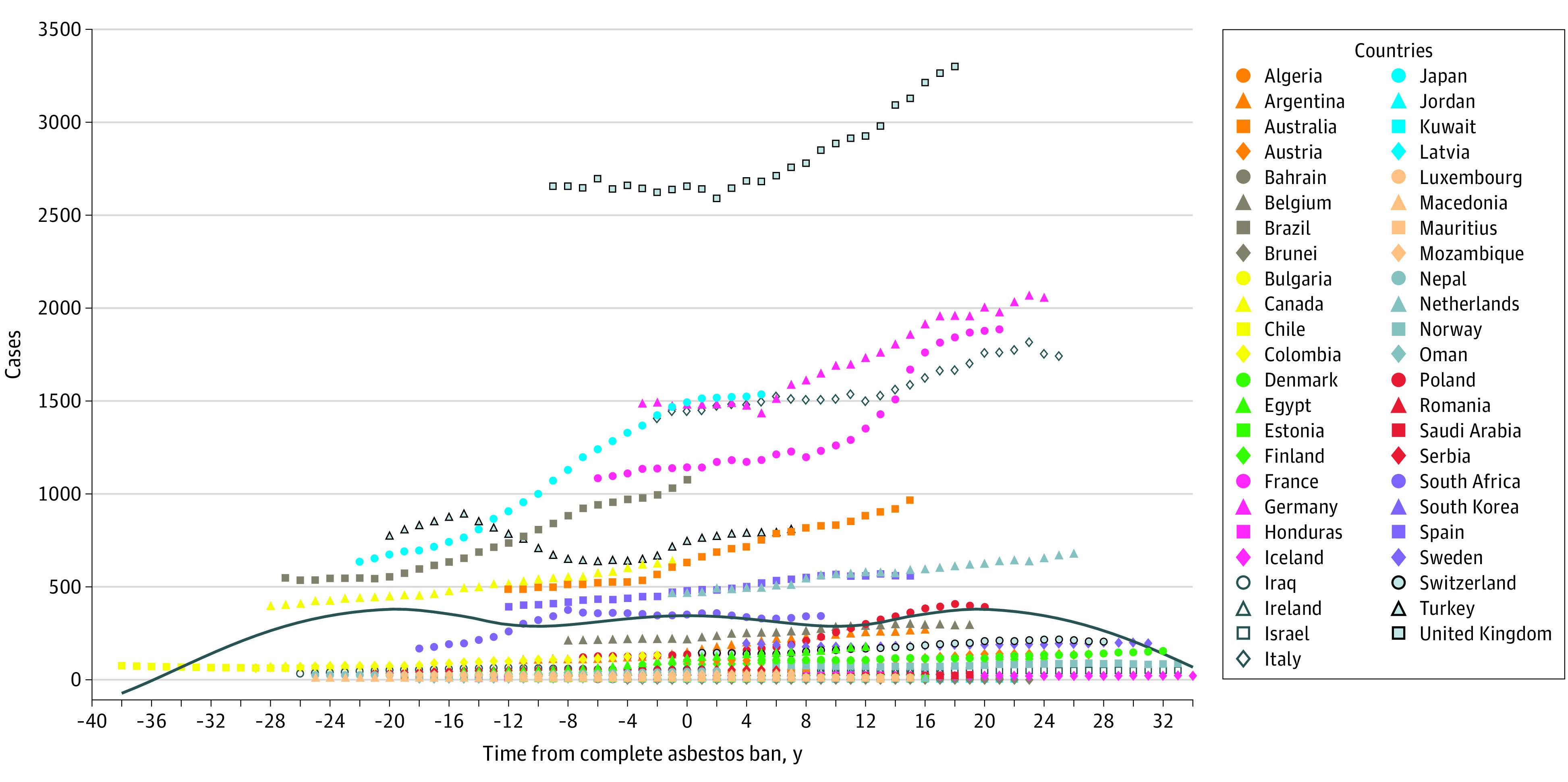
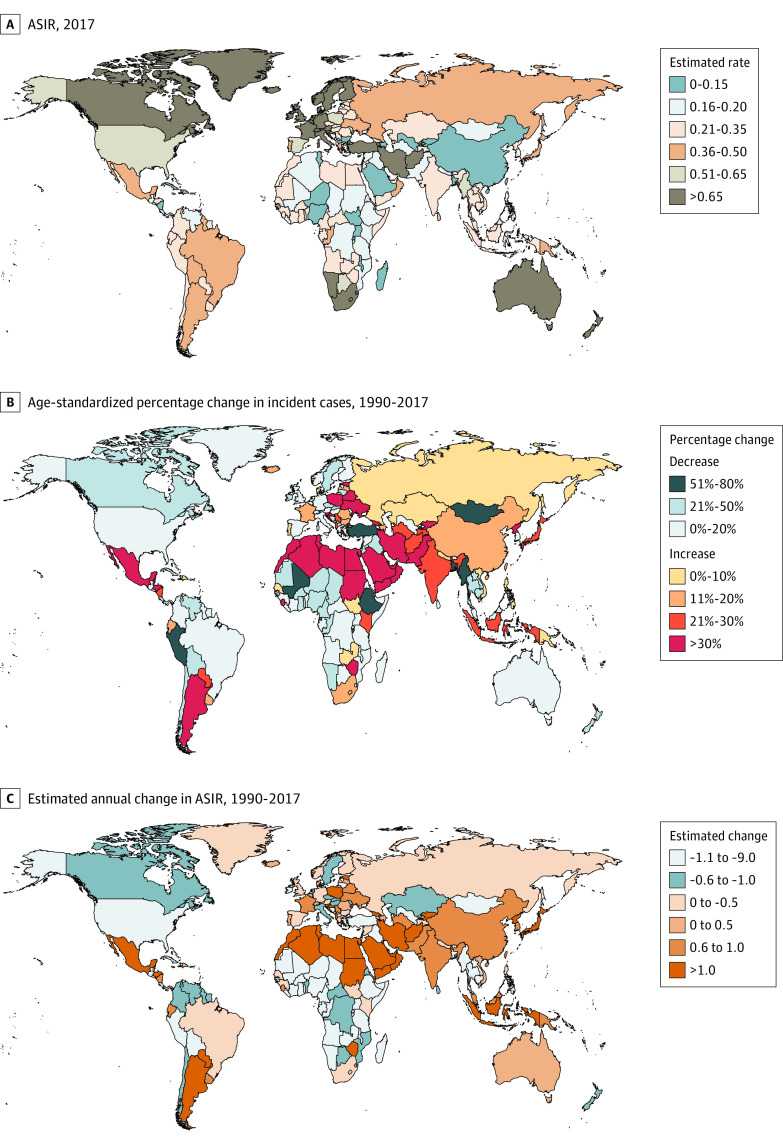
Results: Overall, 34 615 new cases (95% uncertainty interval [UI], 33 530-35 697 cases) of mesothelioma and 29 909 deaths (95% UI, 29 134-30 613 deaths) associated with mesothelioma were identified in 2017, and more than 70% of these cases and deaths were among male individuals. In 1990, the number of incident cases was 21 224 (95% UI, 17 503-25 450), and the number of deaths associated with mesothelioma was 17 406 (95% UI, 14 495-20 660). These numbers increased worldwide from 1990 to 2017, with more than 50% of cases recorded in regions with high SDI levels, whereas the age-standardized incidence rate (from 0.52 [95% UI, 0.43-0.62] in 1990 to 0.44 [95% UI, 0.42-0.45] in 2017) and the age-standardized death rate (from 0.44 [95% UI, 0.37-0.52] in 1990 to 0.38 [95% UI, 0.37-0.39] in 2017) decreased, with estimated annual percentage changes of -0.61 (95% CI, -0.67 to -0.54) for age-standardized incidence rate and -0.44 (95% CI, -0.52 to -0.37) for age-standardized death rate. The proportion of incident cases among those 70 years or older continued to increase (from 36.49% in 1990 to 44.67% in 2017), but the proportion of patients younger than 50 years decreased (from 16.74% in 1990 to 13.75% in 2017) over time. In addition, mesothelioma incident cases and age-standardized incidence rates began to decrease after 20 years of a complete ban on asbestos use. For example, in Italy, a complete ban on asbestos went into effect in 1992; incident cases increased from 1409 individuals (95% UI, 1013-1733 individuals) in 1990, peaked in 2015 after 23 years of the asbestos ban, then decreased from 1820 individuals (95% UI, 1699-1981 individuals) in 2015 to 1746 individuals (95% UI, 1555-1955 individuals) in 2017.
Conclusions and relevance: This cross-sectional study found that incident cases of mesothelioma and deaths associated with mesothelioma continuously increased worldwide, especially in resource-limited regions with low SDI levels. Based on these findings, global governments and medical institutions may consider formulating optimal policies and strategies for the targeted prevention and management of mesothelioma.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
