

Pharmacological and non-pharmacological interventions to prevent delirium in critically ill patients: a systematic review and network meta-analysis
- PMID: 34379152
- PMCID: PMC8356549
- DOI: 10.1007/s00134-021-06490-3
Pharmacological and non-pharmacological interventions to prevent delirium in critically ill patients: a systematic review and network meta-analysis
Abstract
Purpose: To compare the effects of prevention interventions on delirium occurrence in critically ill adults.
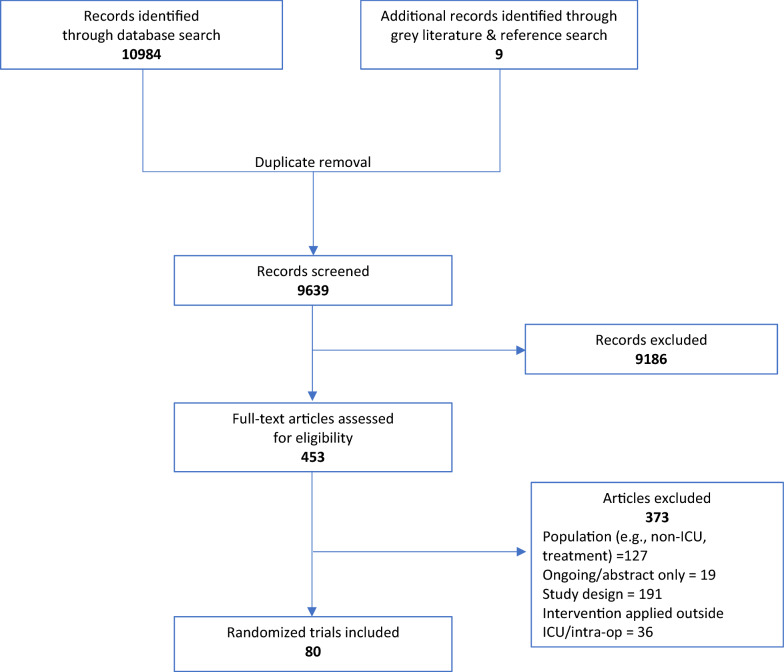
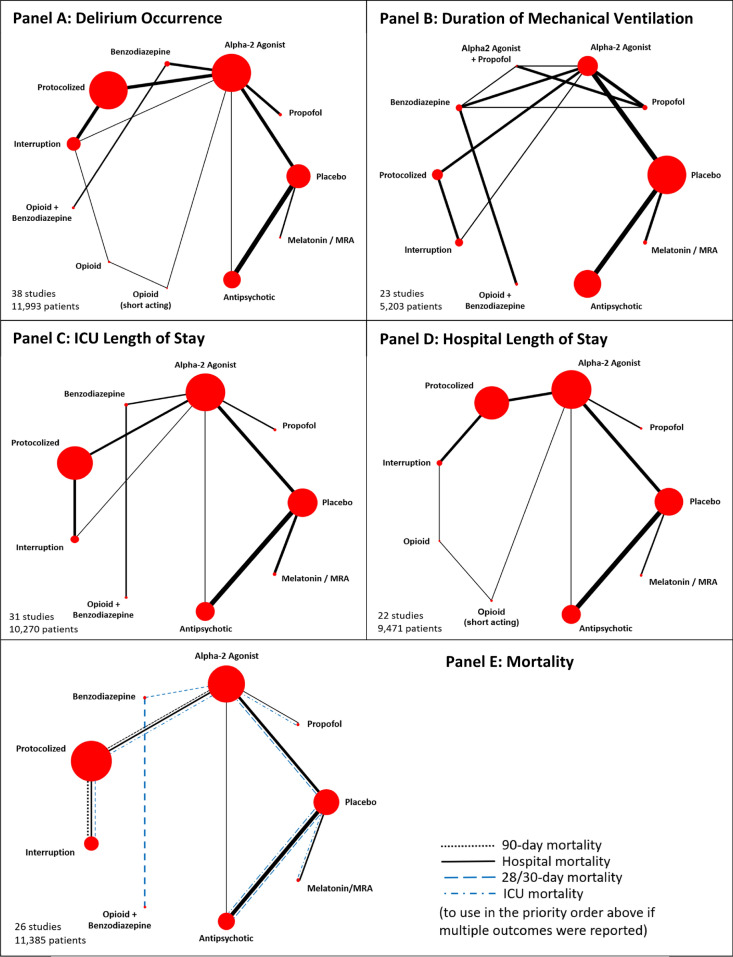
Methods: MEDLINE, Embase, PsychINFO, CINAHL, Web of Science, Cochrane Library, Prospero, and WHO international clinical trial registry were searched from inception to April 8, 2021. Randomized controlled trials of pharmacological, sedation, non-pharmacological, and multi-component interventions enrolling adult critically ill patients were included. We performed conventional pairwise meta-analyses, NMA within Bayesian random effects modeling, and determined surface under the cumulative ranking curve values and mean rank. Reviewer pairs independently extracted data, assessed bias using Cochrane Risk of Bias tool and evidence certainty with GRADE. The primary outcome was delirium occurrence; secondary outcomes were durations of delirium and mechanical ventilation, length of stay, mortality, and adverse effects.
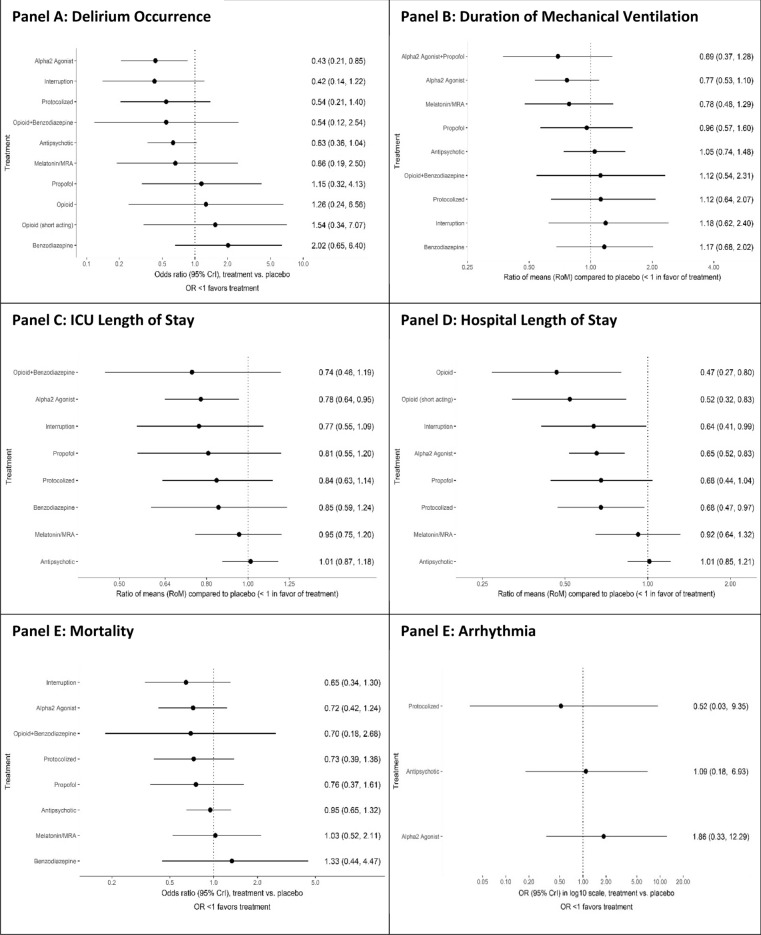
Results: Eighty trials met eligibility criteria: 67.5% pharmacological, 31.3% non-pharmacological and 1.2% mixed pharmacological and non-pharmacological interventions. For delirium occurrence, 11 pharmacological interventions (38 trials, N = 11,993) connected to the evidence network. Compared to placebo, only dexmedetomidine (21/22 alpha2 agonist trials were dexmedetomidine) probably reduces delirium occurrence (odds ratio (OR) 0.43, 95% Credible Interval (CrI) 0.21-0.85; moderate certainty). Compared to benzodiazepines, dexmedetomidine (OR 0.21, 95% CrI 0.08-0.51; low certainty), sedation interruption (OR 0.21, 95% CrI 0.06-0.69; very low certainty), opioid plus benzodiazepine (OR 0.27, 95% CrI 0.10-0.76; very low certainty), and protocolized sedation (OR 0.27, 95% CrI 0.09-0.80; very low certainty) may reduce delirium occurrence but the evidence is very uncertain. Dexmedetomidine probably reduces ICU length of stay compared to placebo (Ratio of Means (RoM) 0.78, CrI 0.64-0.95; moderate certainty) and compared to antipsychotics (RoM 0.76, CrI 0.61-0.98; low certainty). Sedative interruption, protocolized sedation and opioids may reduce hospital length of stay compared to placebo, but the evidence is very uncertain. No intervention influenced mechanical ventilation duration, mortality, or arrhythmia. Single and multi-component non-pharmacological interventions did not connect to any evidence networks to allow for ranking and comparisons as planned; pairwise comparisons did not detect differences compared to standard care.
Conclusion: Compared to placebo and benzodiazepines, we found dexmedetomidine likely reduced the occurrence of delirium in critically ill adults. Compared to benzodiazepines, sedation-minimization strategies may also reduce delirium occurrence, but the evidence is uncertain.
Keywords: Critical care; Delirium; Non-pharmacological interventions; Pharmacological; Prevention.
© 2021. Springer-Verlag GmbH Germany, part of Springer Nature.
Conflict of interest statement
All the authors declare no support from any organization for the submitted work; no financial relationships with any organizations that might have an interest in the submitted work in the previous 3 years; no other relationships or activities that could appear to have influenced the submitted work. BH has previously provided methodologic advice to Eversana Inc for the conduct of systemic reviews and meta-analysis on unrelated topics.
Figures
References
-
- Devlin JW, Skrobik Y, Gelinas C, Needham DM, Slooter AJC, Pandharipande PP, Watson PL, Weinhouse GL, Nunnally ME, Rochwerg B, Balas MC, van den Boogaard M, Bosma KJ, Brummel NE, Chanques G, Denehy L, Drouot X, Fraser GL, Harris JE, Joffe AM, Kho ME, Kress JP, Lanphere JA, McKinley S, Neufeld KJ, Pisani MA, Payen JF, Pun BT, Puntillo KA, Riker RR, Robinson BRH, Shehabi Y, Szumita PM, Winkelman C, Centofanti JE, Price C, Nikayin S, Misak CJ, Flood PD, Kiedrowski K, Alhazzani W. Clinical practice guidelines for the prevention and management of pain, agitation/sedation, delirium, immobility, and sleep disruption in adult patients in the ICU. Crit Care Med. 2018;46:e825–e873. doi: 10.1097/CCM.0000000000003299. - DOI - PubMed
-
- Fraser GL, Devlin JW, Worby CP, Alhazzani W, Barr J, Dasta JF, Kress JP, Davidson JE, Spencer FA. Benzodiazepine versus nonbenzodiazepine-based sedation for mechanically ventilated, critically ill adults: a systematic review and meta-analysis of randomized trials. Crit Care Med. 2013;41:S30–38. doi: 10.1097/CCM.0b013e3182a16898. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
