

Assessing early child development and its association with stunting and schistosome infections in rural Zimbabwean children using the Griffiths Scales of Child Development
- PMID: 34379618
- PMCID: PMC8357151
- DOI: 10.1371/journal.pntd.0009660
Assessing early child development and its association with stunting and schistosome infections in rural Zimbabwean children using the Griffiths Scales of Child Development
Abstract
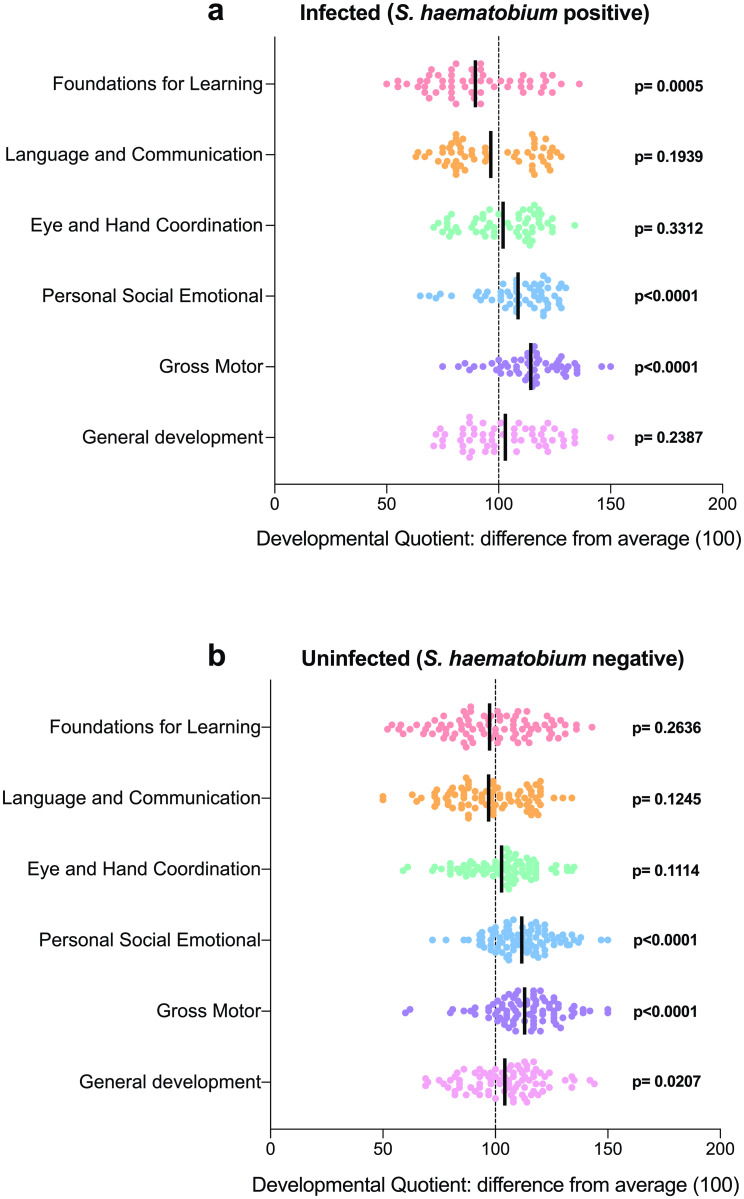
There is a paucity of reference early childhood development (ECD) data at community level in rural Africa. Our objective was to conduct a comprehensive assessment of ECD in rural Zimbabwe and determine the impact of stunting and schistosome infections on ECD. Using the Griffiths Scales of Child Development, we conducted a cross sectional assessment of Eye and Hand Coordination (EHC), Personal-Social-Emotional (PSE), Language and Communication (LC), Foundations of Learning (FL) and Gross Motor (GM) domains and the summary General Development (GD) in 166 children aged 6-72 months. The effects of stunting, malnutrition and Schistosoma haematobium infection on ECD was determined. The impact of praziquantel curative treatment of schistosome infection on the developmental scores was determined through a longitudinal follow up at 6 and 12 months. From an initial 166 children, 11 were found to have developmental deficits warranting further investigation. Of the remaining 155, 58.7% recorded a good (≥ average) score for the overall General Development (GD). Proportions of children scoring above the cut-off (≥ average) for each domain were GM (84.5%), PSE (80.6%), EHC (61.9%), FL (43.9%) and LC (44.5%). The prevalence of stunting was 26.8% (95% CI = 20.1%-34.8%) Scores for stunted children were significantly lower for EHC (p = 0.0042), GM (p = 0.0099), and GD (p = 0.0014) with the fraction of lower scores attributable to stunting being GM = 63.4%, GD = 46.6%, EHC = 45%, and LC = 21%. S. haematobium infection prevalence was 39.7% and mean infection intensity was 5.4 eggs/10 ml urine. Infected children had poorer cognitive performance scores for the FL (p = 0.0005) with 30.8% of poor FL attributable to the infection. Performance in all domains improved to the expected normal or above reference levels at 6 and 12 months post curative treatment of schistosome infections. Our study documented reference values for ECD in rural Zimbabwean children. The study detected deficiencies in the FL domain, which were more pronounced in children, infected with schistosomes, highlighting the need for provision of cognitive stimulation tools and access to early childhood foundation education. There is also need for improved child nutrition and treatment of schistosome infections to improve child development outcomes.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures





References
-
- Blouin B, Casapia M, Joseph L, Gyorkos TW. A longitudinal cohort study of soil-transmitted helminth infections during the second year of life and associations with reduced long-term cognitive and verbal abilities. PLoS Negl Trop Dis. 2018;12(7):e0006688. doi: 10.1371/journal.pntd.0006688. - DOI - PMC - PubMed
-
- Pabalan N, Singian E, Tabangay L, Jarjanazi H, Boivin MJ, Ezeamama AE. Soil-transmitted helminth infection, loss of education and cognitive impairment in school-aged children: A systematic review and meta-analysis. PLoS Negl Trop Dis. 2018;12(1):e0005523. Epub 2018/01/13. doi: 10.1371/journal.pntd.0005523. - DOI - PMC - PubMed
