

Case-area targeted interventions (CATI) for reactive dengue control: Modelling effectiveness of vector control and prophylactic drugs in Singapore
- PMID: 34379641
- PMCID: PMC8357181
- DOI: 10.1371/journal.pntd.0009562
Case-area targeted interventions (CATI) for reactive dengue control: Modelling effectiveness of vector control and prophylactic drugs in Singapore
Abstract
Background: Targeting interventions to areas that have recently experienced cases of disease is one strategy to contain outbreaks of infectious disease. Such case-area targeted interventions (CATI) have become an increasingly popular approach for dengue control but there is little evidence to suggest how precisely targeted or how recent cases need to be, to mount an effective response. The growing interest in the development of prophylactic and therapeutic drugs for dengue has also given new relevance for CATI strategies to interrupt transmission or deliver early treatment.
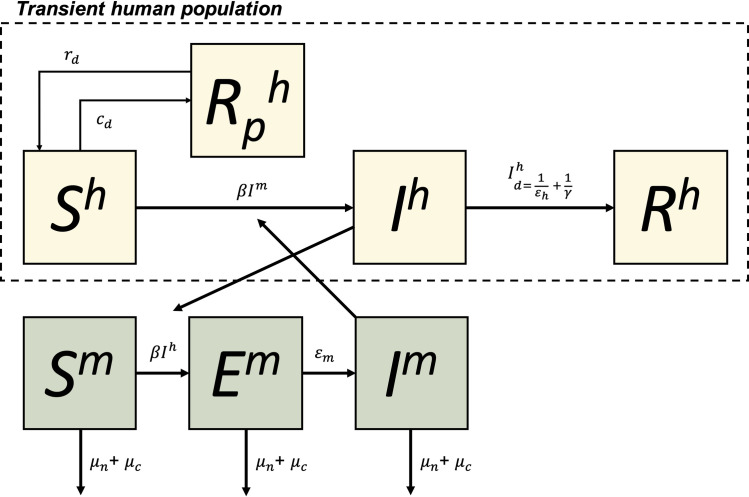
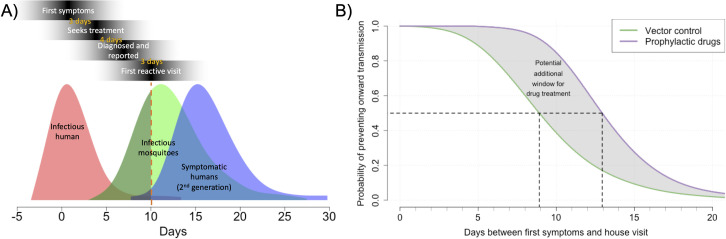
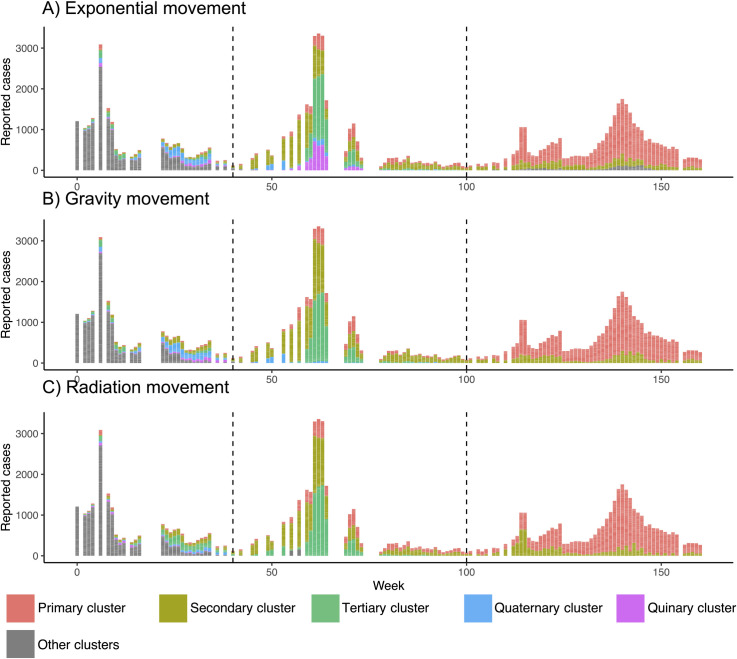
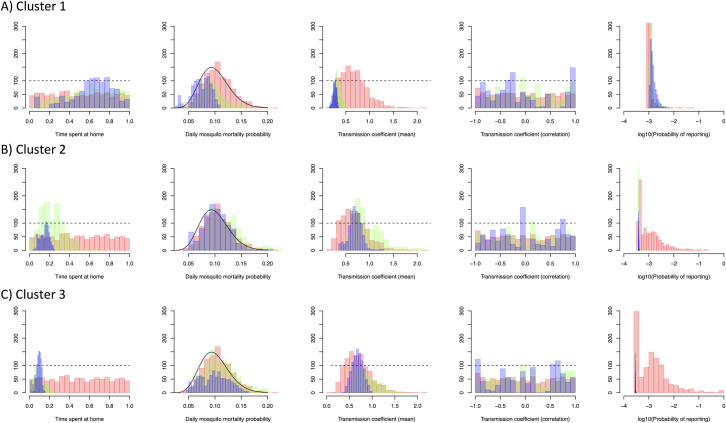
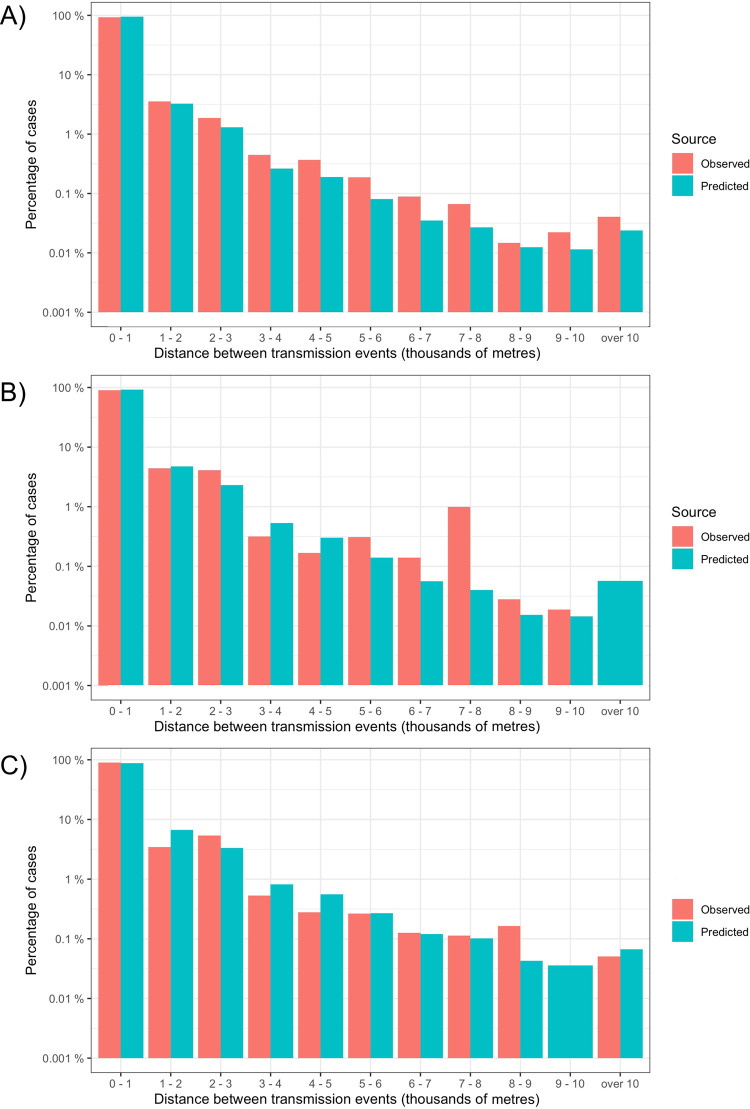
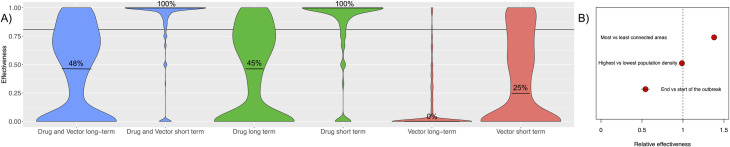
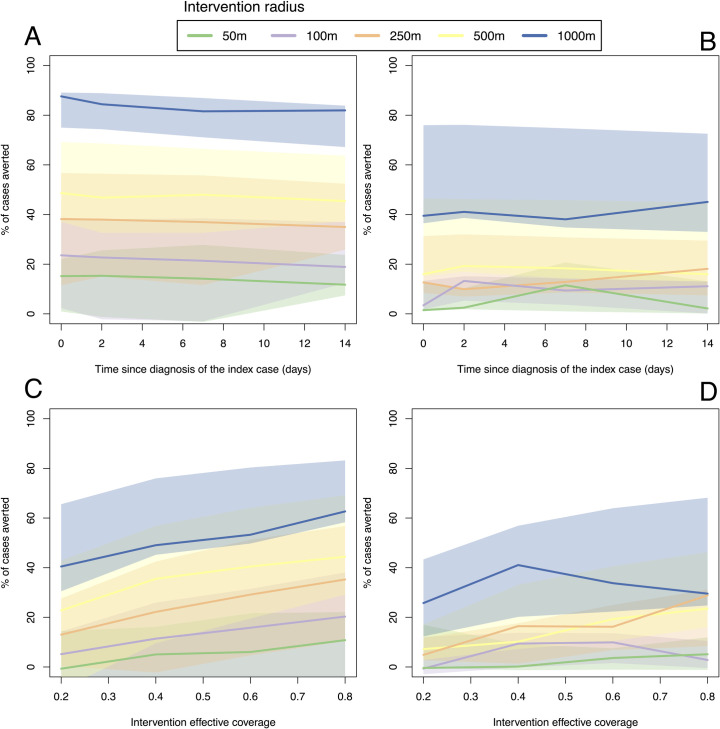
Methods/principal findings: Here we develop a patch-based mathematical model of spatial dengue spread and fit it to spatiotemporal datasets from Singapore. Simulations from this model suggest CATI strategies could be effective, particularly if used in lower density areas. To maximise effectiveness, increasing the size of the radius around an index case should be prioritised even if it results in delays in the intervention being applied. This is partially because large intervention radii ensure individuals receive multiple and regular rounds of drug dosing or vector control, and thus boost overall coverage. Given equivalent efficacy, CATIs using prophylactic drugs are predicted to be more effective than adult mosquito-killing vector control methods and may even offer the possibility of interrupting individual chains of transmission if rapidly deployed. CATI strategies quickly lose their effectiveness if baseline transmission increases or case detection rates fall.
Conclusions/significance: These results suggest CATI strategies can play an important role in dengue control but are likely to be most relevant for low transmission areas where high coverage of other non-reactive interventions already exists. Controlled field trials are needed to assess the field efficacy and practical constraints of large operational CATI strategies.
Conflict of interest statement
I have read the journal’s policy and the authors of this manuscript have the following competing interests: MVL, GHT and JM are employees of Johnson & Johnson. LS and LN are employees of the Singapore national Environment Agency
Figures

References
-
- World Health Organization. Dengue guidelines for diagnosis, treatment, prevention and control: new edition. 2009. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
