

Testing telediagnostic right upper quadrant abdominal ultrasound in Peru: A new horizon in expanding access to imaging in rural and underserved areas
- PMID: 34379679
- PMCID: PMC8357175
- DOI: 10.1371/journal.pone.0255919
Testing telediagnostic right upper quadrant abdominal ultrasound in Peru: A new horizon in expanding access to imaging in rural and underserved areas
Abstract
Background: Hepatic and biliary diseases are prevalent worldwide, but the majority of people lack access to diagnostic medical imaging for their assessment. The liver and gallbladder are readily amenable to sonographic examination, and ultrasound is a portable, cost-effective imaging modality suitable for use in rural and underserved areas. However, the deployment of ultrasound in these settings is limited by the lack of experienced sonographers to perform the exam. In this study, we tested an asynchronous telediagnostic system for right upper quadrant abdominal ultrasound examination operated by individuals without prior ultrasound experience to facilitate deployment of ultrasound to rural and underserved areas.
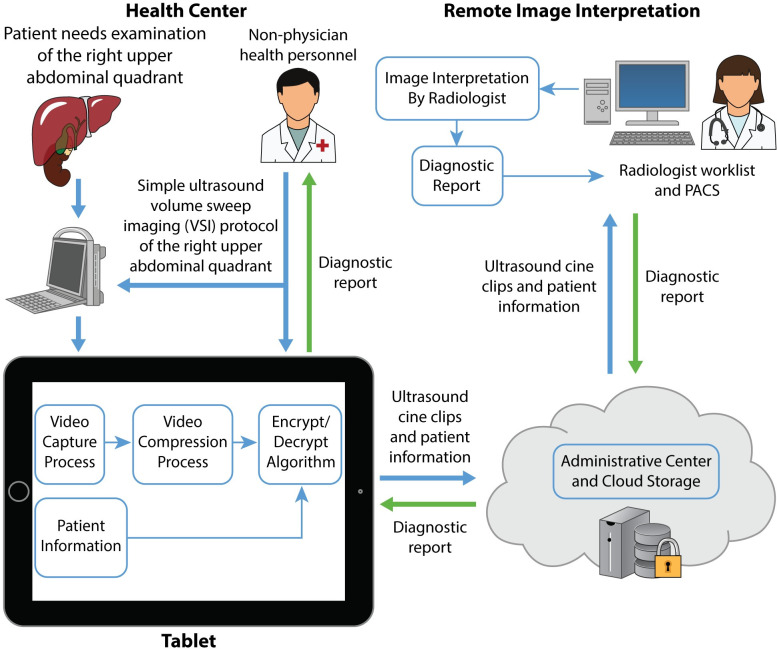
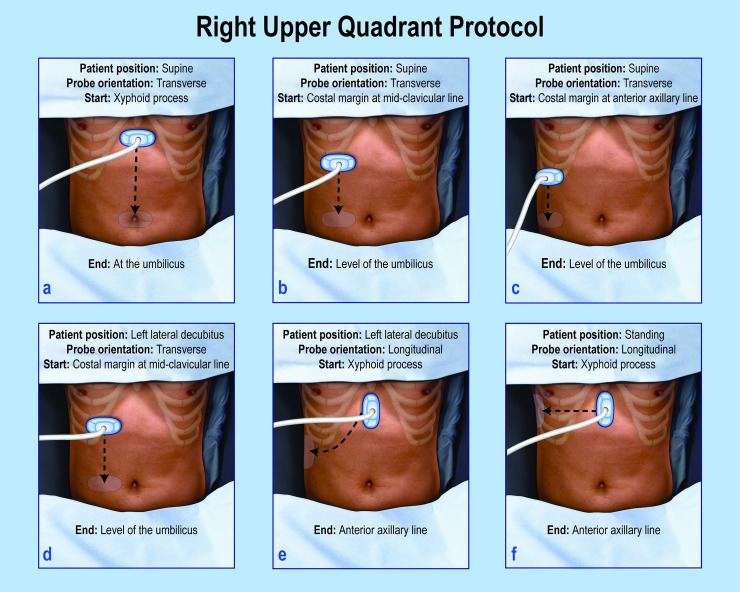
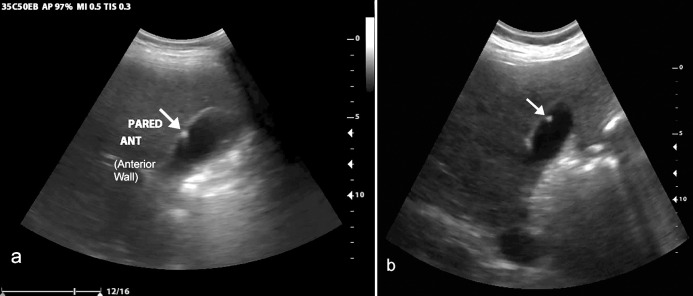
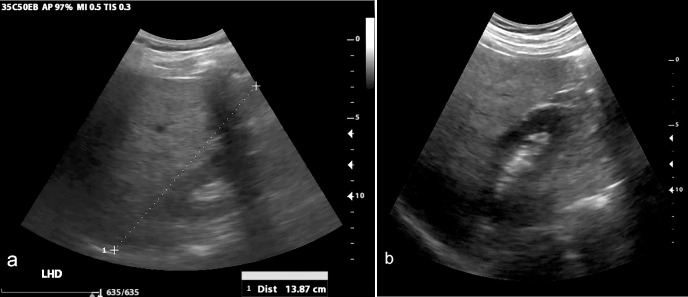
Methods: The teleultrasound system utilized in this study employs volume sweep imaging and a telemedicine app installed on a tablet which connects to an ultrasound machine. Volume sweep imaging is an ultrasound technique in which an individual scans the target region utilizing preset ultrasound sweeps demarcated by easily recognized external body landmarks. The sweeps are saved as video clips for later interpretation by an experienced radiologist. Teleultrasound scans from a Peruvian clinic obtained by individuals without prior ultrasound experience were sent to the United States for remote interpretation and quality assessment. Standard of care comparison was made to a same-day ultrasound examination performed by a radiologist.
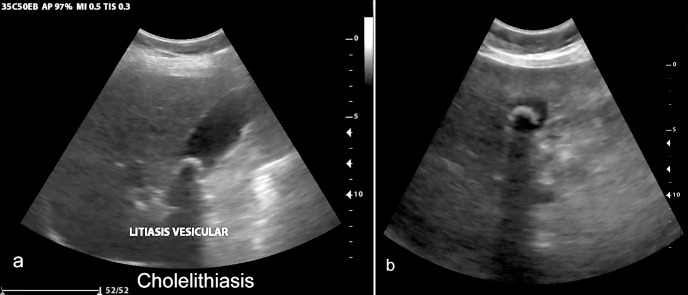
Results: Individuals without prior ultrasound experience scanned 144 subjects. Image quality was rated "poor" on 36.8% of exams, "acceptable" on 38.9% of exams, and "excellent" on 24.3% of exams. Among telemedicine exams of "acceptable" or "excellent" image quality (n = 91), greater than 80% of the liver and gallbladder were visualized in the majority of cases. In this group, there was 95% agreement between standard of care and teleultrasound on whether an exam was normal or abnormal, with a Cohen's kappa of 0.84 (95% CI 0.7-0.98, p <0.0001). Finally, among these teleultrasound exams of "acceptable" or "excellent" image quality, the sensitivity for cholelithiasis was 93% (95% CI 68.1%-99.8%), and the specificity was 97% (95% CI 89.5%-99.6%).
Conclusion: This asynchronous telediagnostic system allows individuals without prior ultrasound experience to effectively scan the liver, gallbladder, and right kidney with a high degree of agreement with standard of care ultrasound. This system can be deployed to improve access to diagnostic imaging in low-resource areas.
Conflict of interest statement
The authors have read the journal’s policy and have the following competing interests: ME, LT, and CC were paid employees of Medical Innovation and Technology during the study period. Medical Innovation and Technology also provided funding for the logistical costs associated with data collection. BC is the founder of and has a financial stake in Medical Innovation and Technology. This company seeks to bring ultrasound to rural areas through telemedicine. The authors would like to declare the following marketed product associated with this research: “Medical for Ultrasound” or “Med4US." This does not alter our adherence to PLOS ONE policies on sharing data and materials. There are no other patents, products in development, or marketed products associated with this research to declare.
Figures
References
-
- Akinyemiju T, Abera S, Ahmed M, Alam N, Alemayohu MA, Allen C, et al. The Burden of Primary Liver Cancer and Underlying Etiologies From 1990 to 2015 at the Global, Regional, and National Level: Results From the Global Burden of Disease Study 2015. JAMA Oncol. 2017;3(12):1683–91. doi: 10.1001/jamaoncol.2017.3055 - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
