

Predicting apneic events in preterm infants using cardio-respiratory and movement features
- PMID: 34380078
- PMCID: PMC8898595
- DOI: 10.1016/j.cmpb.2021.106321
Predicting apneic events in preterm infants using cardio-respiratory and movement features
Abstract
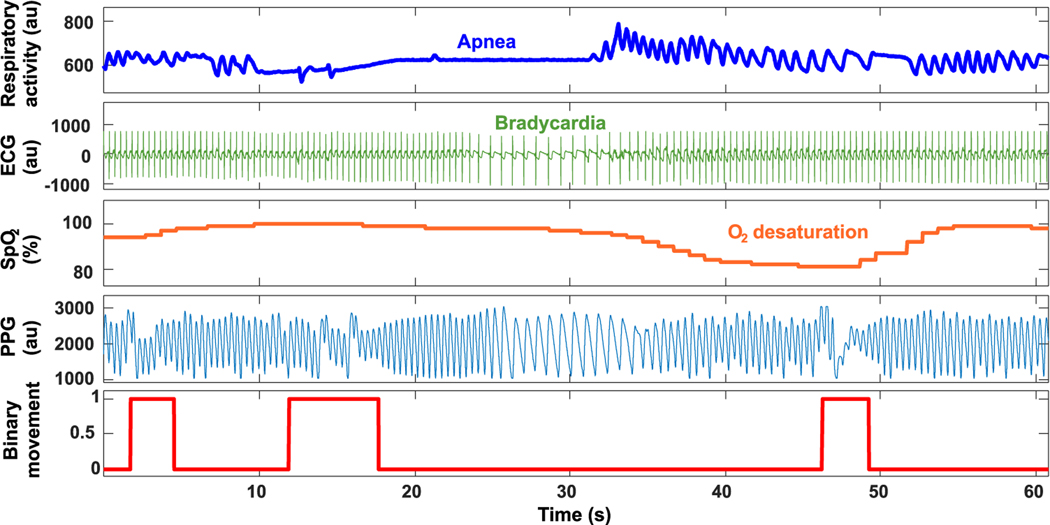
Background and objective: Preterm neonates are prone to episodes of apnea, bradycardia and hypoxia (ABH) that can lead to neurological morbidities or even death. There is broad interest in developing methods for real-time prediction of ABH events to inform interventions that prevent or reduce their incidence and severity. Using advances in machine learning methods, this study develops an algorithm to predict ABH events.
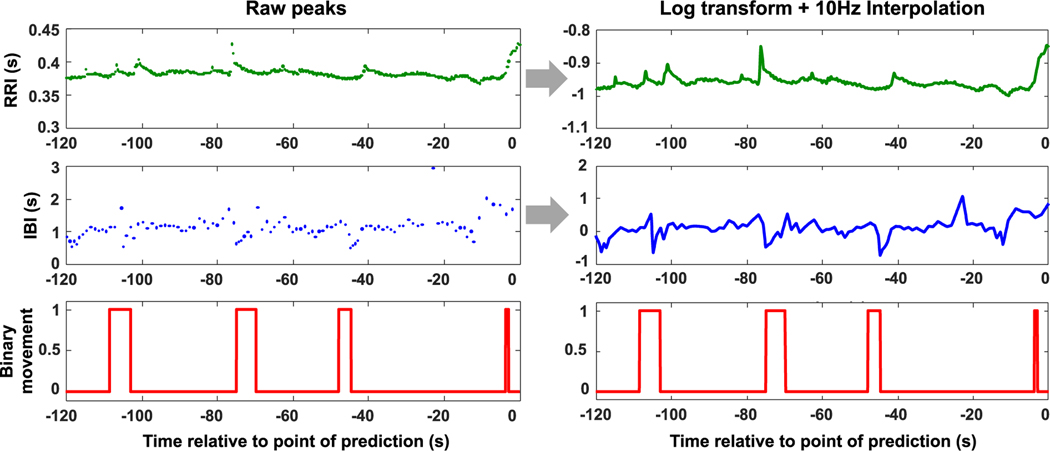
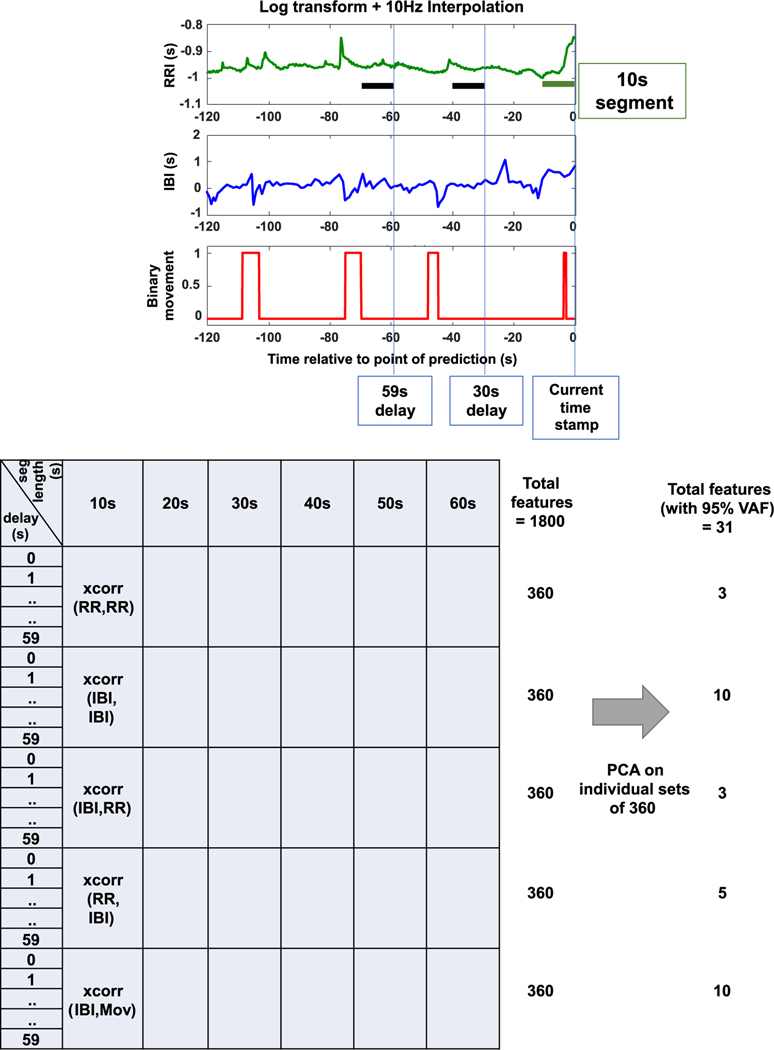
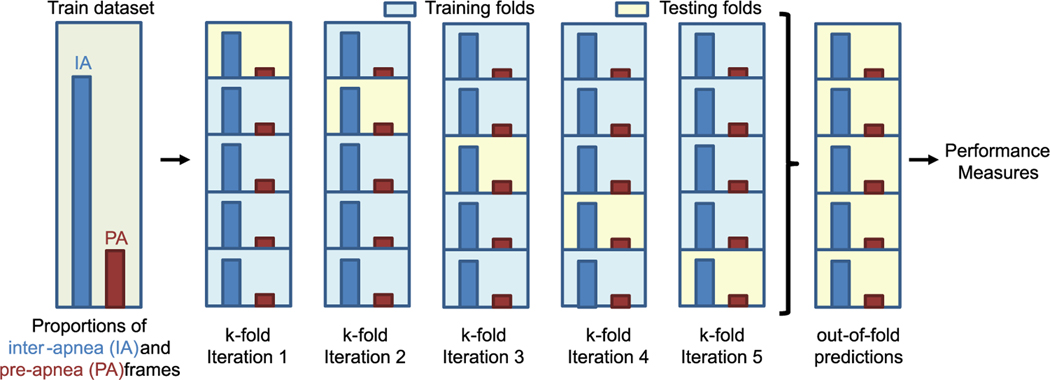
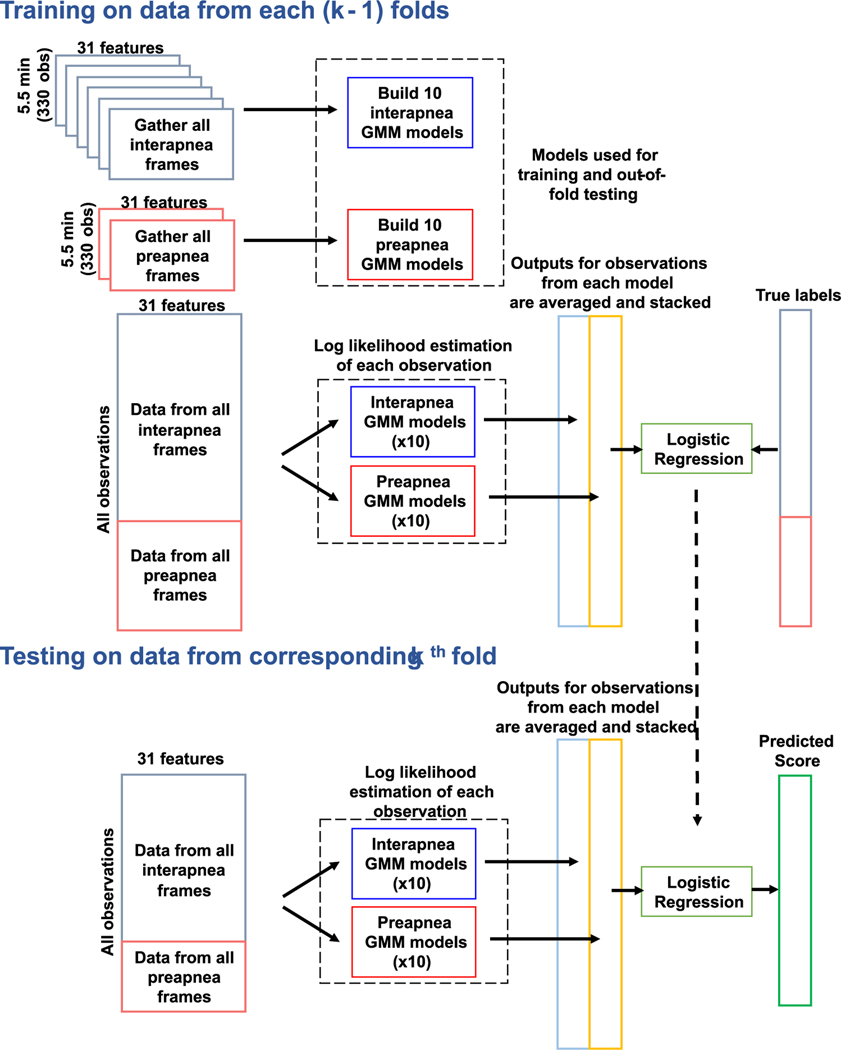
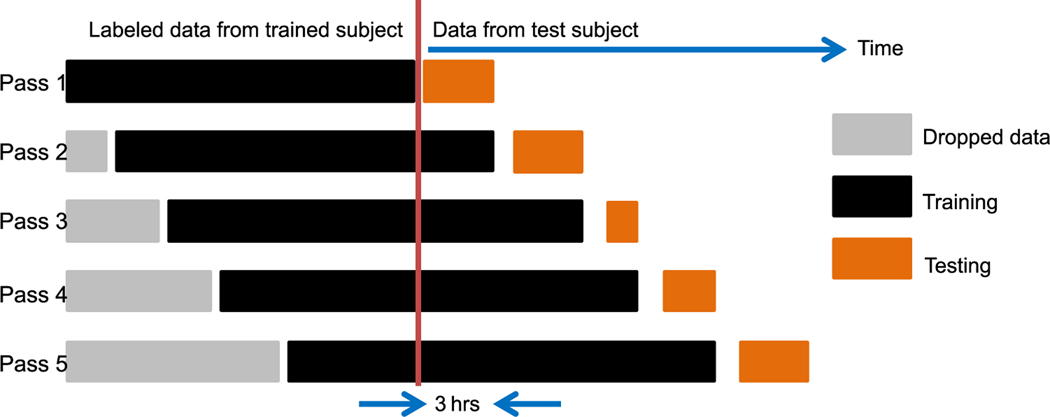
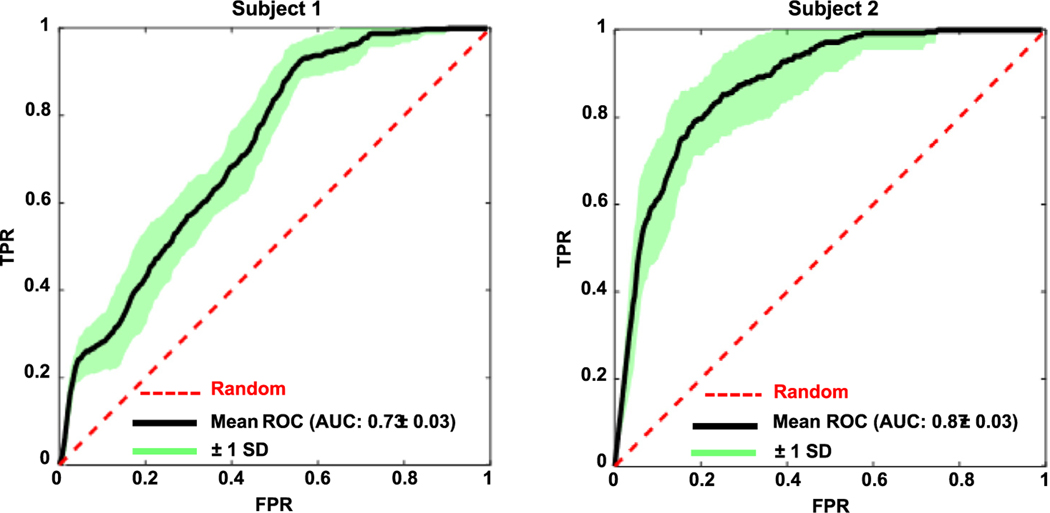
Methods: Following previous studies showing that respiratory instabilities are closely associated with bouts of movement, we present a modeling framework that can predict ABH events using both movement and cardio-respiratory features derived from routine clinical recordings. In 10 preterm infants, movement onsets and durations were estimated with a wavelet-based algorithm that quantified artifactual distortions of the photoplethysmogram signal. For prediction, cardio-respiratory features were created from time-delayed correlations of inter-beat and inter-breath intervals with past values; movement features were derived from time-delayed correlations with inter-breath intervals. Gaussian Mixture Models and Logistic Regression were used to develop predictive models of apneic events. Performance of the models was evaluated with ROC curves.
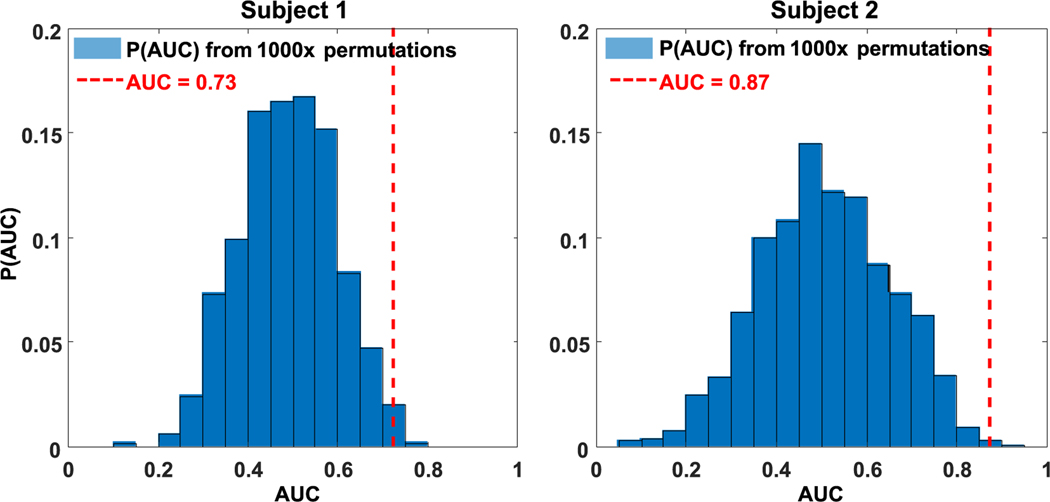
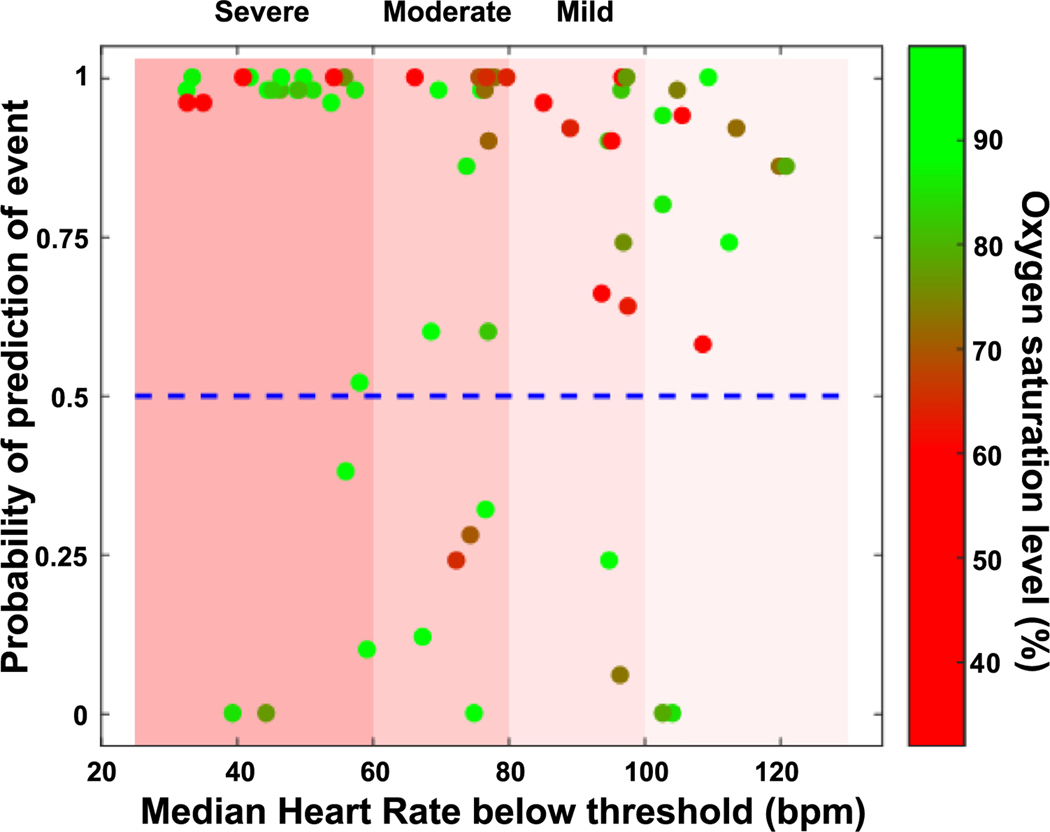
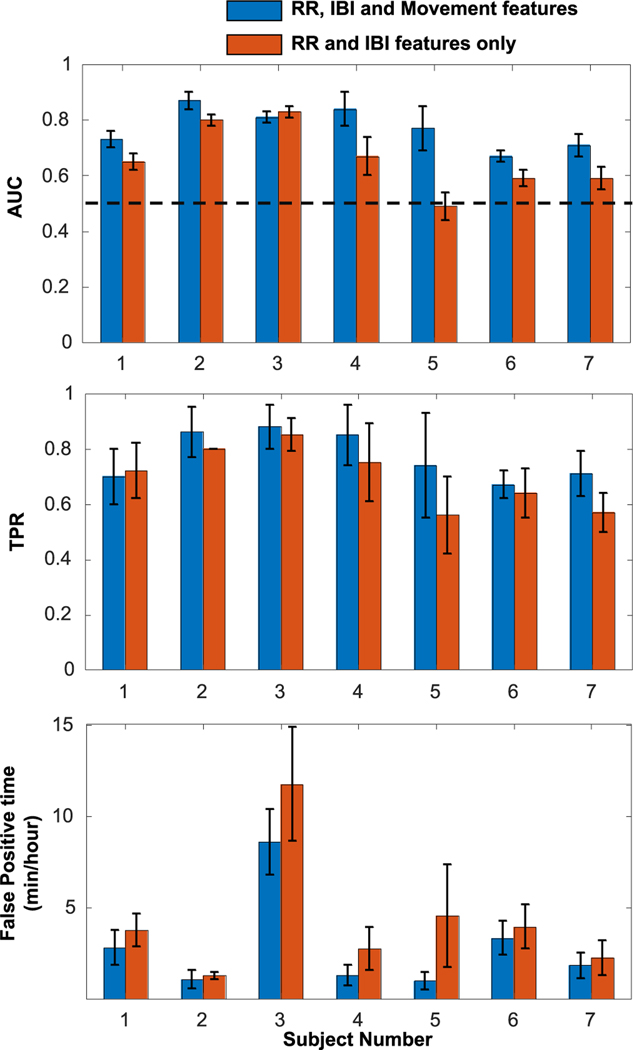
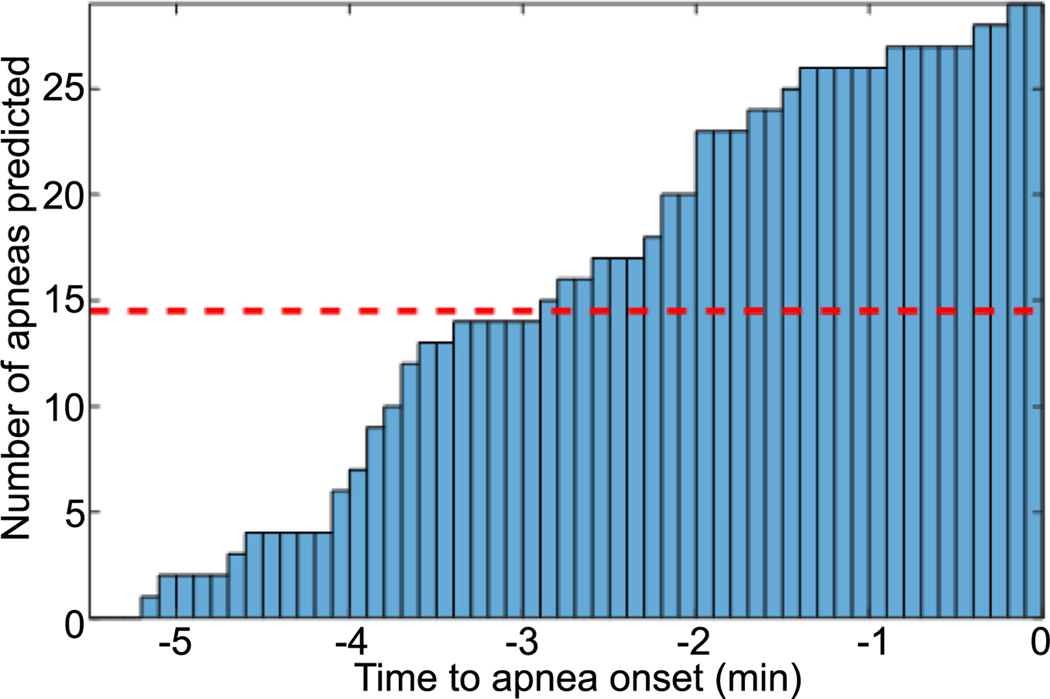
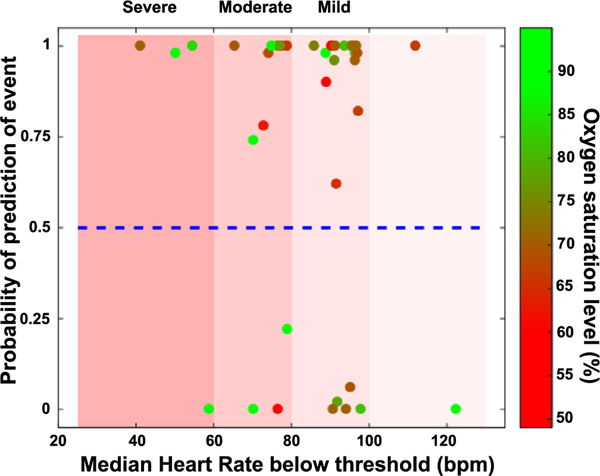
Results: Performance of the prediction framework (mean AUC) was 0.77 ± 0.04 for 66 ABH events on training data from 7 infants. When grouped by the severity of the associated bradycardia during the ABH event, the framework was able to predict 83% and 75% of the most severe episodes in the 7-infant training set and 3-infant test set, respectively. Notably, inclusion of movement features significantly improved the predictions compared with modeling with only cardio-respiratory signals.
Conclusions: Our findings suggest that recordings of movement provide important information for predicting ABH events in preterm infants, and can inform preemptive interventions designed to reduce the incidence and severity of ABH events.
Copyright © 2021. Published by Elsevier B.V.
Conflict of interest statement
Declaration of Competing Interest The authors declare that they have no conflict of interest.
Figures
Similar articles
-
Cardiorespiratory events in preterm infants referred for apnea monitoring studies.Pediatrics. 2001 Dec;108(6):1304-8. doi: 10.1542/peds.108.6.1304. Pediatrics. 2001. PMID: 11731652
-
Improving heart rate estimation in preterm infants with bivariate point process analysis of heart rate and respiration.Annu Int Conf IEEE Eng Med Biol Soc. 2016 Aug;2016:920-923. doi: 10.1109/EMBC.2016.7590851. Annu Int Conf IEEE Eng Med Biol Soc. 2016. PMID: 28268474
-
Undetected episodes of prolonged apnea and severe bradycardia in preterm infants.Pediatrics. 1983 Oct;72(4):541-51. Pediatrics. 1983. PMID: 6889069
-
Neonatal cardiorespiratory monitoring techniques.Semin Neonatol. 2004 Jun;9(3):195-203. doi: 10.1016/j.siny.2003.11.009. Semin Neonatol. 2004. PMID: 15050212 Review.
-
Apnea events in neonatal age: A case report and literature review.Med Hypotheses. 2019 Oct;131:109296. doi: 10.1016/j.mehy.2019.109296. Epub 2019 Jul 3. Med Hypotheses. 2019. PMID: 31443773 Review.
Cited by
-
Comparison of oxygen supplementation in very preterm infants: Variations of oxygen saturation features and their application to hypoxemic episode based risk stratification.Front Pediatr. 2023 Feb 27;11:1016197. doi: 10.3389/fped.2023.1016197. eCollection 2023. Front Pediatr. 2023. PMID: 36923272 Free PMC article.
-
Exploring Computational Techniques in Preprocessing Neonatal Physiological Signals for Detecting Adverse Outcomes: Scoping Review.Interact J Med Res. 2024 Aug 20;13:e46946. doi: 10.2196/46946. Interact J Med Res. 2024. PMID: 39163610 Free PMC article.
-
A nomogram for predicting neonatal apnea: a retrospective analysis based on the MIMIC database.Front Pediatr. 2024 Sep 5;12:1357972. doi: 10.3389/fped.2024.1357972. eCollection 2024. Front Pediatr. 2024. PMID: 39301040 Free PMC article.
-
Continuous sensing and quantification of body motion in infants: A systematic review.Heliyon. 2023 Jul 13;9(7):e18234. doi: 10.1016/j.heliyon.2023.e18234. eCollection 2023 Jul. Heliyon. 2023. PMID: 37501976 Free PMC article. Review.
-
Bradycardia May Decrease Cardiorespiratory Coupling in Preterm Infants.Entropy (Basel). 2023 Dec 3;25(12):1616. doi: 10.3390/e25121616. Entropy (Basel). 2023. PMID: 38136496 Free PMC article.
References
-
- Daily WJR, Klaus M, Belton H, Meyer P, Apnea in premature infants: monitoring, incidence, heart rate changes, and an effect of environmental temperature, Pediatrics 43 (1969) 510–518. - PubMed
-
- Martin RJ, Wilson CG, Apnea of prematurity, Comprehensive Physiol. 2 (2012) 2923–2931. - PubMed
-
- Mathew OP, Apnea of prematurity: pathogenesis and management strategies, J. Perinatol. 31 (2011) 302–310. - PubMed
-
- Shannon DC, Pathophysiologic mechanisms causing sleep apnea and hypoventilation in infants, Sleep 3 (1980) 343–349. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
