

Lessons learned from Integrated Management Program Advancing Community Treatment of Atrial Fibrillation (IMPACT-AF): a pragmatic clinical trial of computerized decision support in primary care
- PMID: 34380542
- PMCID: PMC8359062
- DOI: 10.1186/s13063-021-05488-y
Lessons learned from Integrated Management Program Advancing Community Treatment of Atrial Fibrillation (IMPACT-AF): a pragmatic clinical trial of computerized decision support in primary care
Erratum in
-
Correction: Lessons learned from Integrated Management Program Advancing Community Treatment of Atrial Fibrillation (IMPACT-AF): a pragmatic clinical trial of computerized decision support in primary care.Trials. 2022 Jul 5;23(1):547. doi: 10.1186/s13063-022-06484-6. Trials. 2022. PMID: 35790974 Free PMC article. No abstract available.
Abstract
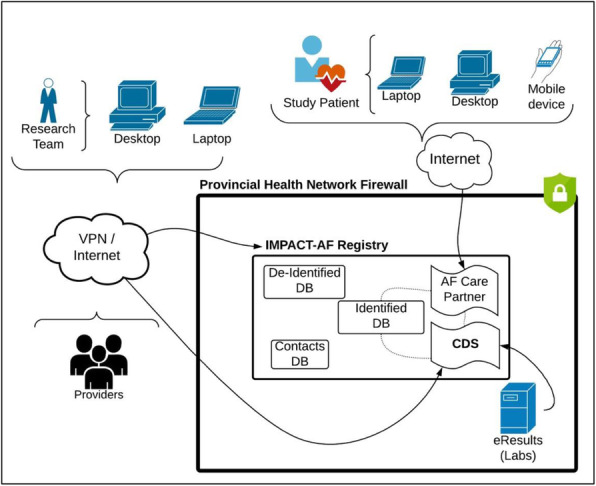
Background: Integrated Management Program Advancing Community Treatment of Atrial Fibrillation (IMPACT-AF) was a pragmatic, cluster randomized trial assessing the effectiveness of a clinical decision support (CDS) tool in primary care, Nova Scotia, Canada. We evaluated if CDS software versus Usual Care could help primary care providers (PCPs) deliver individualized guideline-based AF patient care.
Methods: Key study challenges including CDS development and implementation, recruitment, and data integration documented over the trial duration are presented as lessons learned.
Results: Adequate resources must be allocated for software development, updates and feasibility testing. Development took longer than projected. End-user feedback suggested network access and broadband speeds impeded uptake; they felt further that the CDS was not sufficiently user-friendly or efficient in supporting AF care (i.e., repetitive alerts). Integration across e-platforms is crucial. Intellectual property and other issues prohibited CDS integration within electronic medical records and provincial e-health platforms. Double login and data entry were impediments to participation or reasons for provider withdrawal. Data integration challenges prevented easy and timely data access, analysis, and reporting. Primary care study recruitment is resource intensive. Altogether, 203 PCPs and 1145 of their patients participated, representing 25% of eligible providers and 12% of AF patients in Nova Scotia, respectively. The most effective provider recruitment strategy was in-office, small group lunch-and-learns. PCPs with past research experience or who led patient consent were top recruiters. The study office played a pivotal role in achieving patient recruitment targets.
Conclusions: A rapid growth in healthcare data is leading to widespread development of CDS. Our experience found practical issues to address for such applications to succeed. Feasibility testing to assess the utility of any healthcare CDS prior to implementation is recommended. Adequate resources are necessary to support successful recruitment for future pragmatic trials. CDS tools that integrate multiple co-morbid guidelines across eHealth platforms should be pursued.
Trial registration: ClinicalTrials.gov NCT01927367. Registered on August 22, 2013.
Keywords: Atrial fibrillation; Clinical decision support; Clinical trials; Informatics.
© 2021. The Author(s).
Conflict of interest statement
J. C. reports grants from Bayer Inc. during the conduct of the study and personal fees from Bayer, Servier, and HLS Therapeutic, outside the submitted work. R.P. reports grants from Bayer and Pfizer during the conduct of the study. J.M.K. reports other fees from Merck Canada, Bayer, and Pfizer outside the submitted work. A.C. and S.H.C. are employees of Bayer Inc. J.N.W. reports personal fees from Nova Scotia Health Authority during the conduct of the study. All other authors declare no competing interests.
Figures

References
-
- Benjamin EJ, Blaha MJ, Chiuve SE, Cushman M, Das SR, Deo R, de Ferranti SD, Floyd J, Fornage M, Gillespie C, Isasi CR, Jiménez MC, Jordan LC, Judd SE, Lackland D, Lichtman JH, Lisabeth L, Liu S, Longenecker CT, Mackey RH, Matsushita K, Mozaffarian D, Mussolino ME, Nasir K, Neumar RW, Palaniappan L, Pandey DK, Thiagarajan RR, Reeves MJ, Ritchey M, Rodriguez CJ, Roth GA, Rosamond WD, Sasson C, Towfighi A, Tsao CW, Turner MB, Virani SS, Voeks JH, Willey JZ, Wilkins JT, Wu JH, Alger HM, Wong SS, Muntner P, American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Heart Disease and Stroke Statistics-2017 Update: A Report From the American Heart Association [published correction appears in Circulation. 2017 Mar 7;135(10 ):e646] [published correction appears in Circulation. 2017 Sep 5;136(10 ):e196]. Circulation. 2017;135(10):e146-e603. doi:10.1161/CIR.0000000000000485, Heart Disease and Stroke Statistics—2017 Update: A Report From the American Heart Association. - PMC - PubMed
-
- Ogilvie IM, Newton N, Welner SA, et al. Underuse of oral anticoagulants in atrial fibrillation: a systematic review. Am J Med Sci. 2010;123(7):638–645.e4. - PubMed
-
- Cox JL, Parkash R, Abidi SR, Thabane L, Xie F, MacKillop J, et al. Optimizing primary care management of atrial fibrillation: the rationale and methods of the Integrated Management Program Advancing Community Treatment of Atrial Fibrillation (IMPACT-AF) study. American Heart Journal. 2018;201:149–57 10.1016/j.ahj.2018.04.008. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
