

A role for Sfrp2 in cardiomyogenesis in vivo
- PMID: 34380738
- PMCID: PMC8379963
- DOI: 10.1073/pnas.2103676118
A role for Sfrp2 in cardiomyogenesis in vivo
Abstract
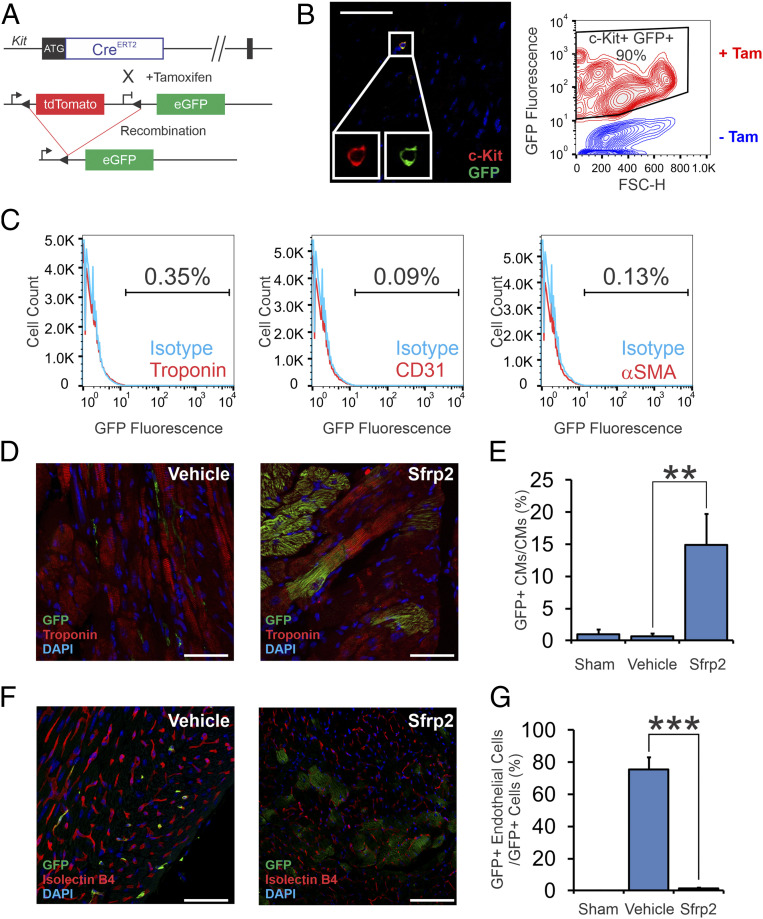
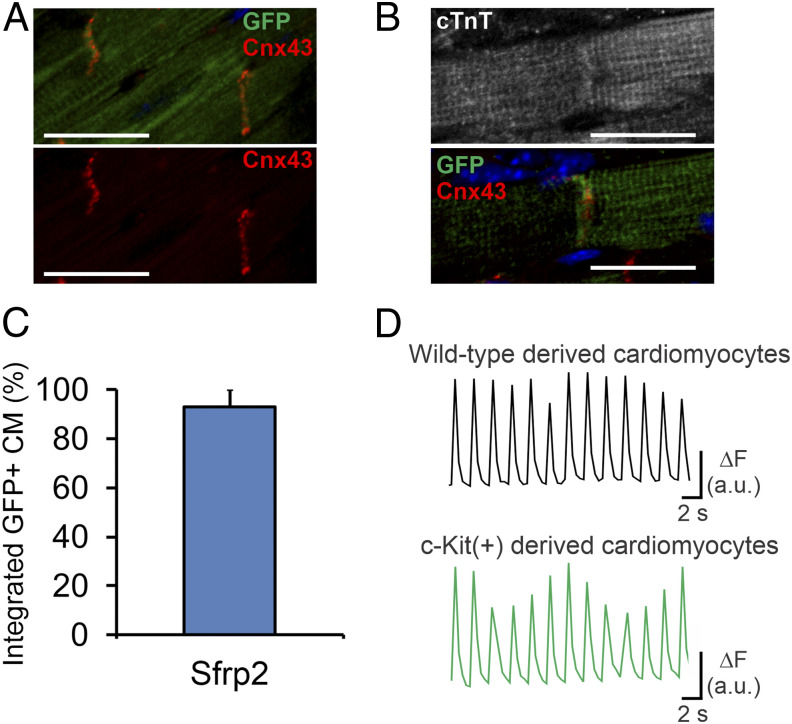
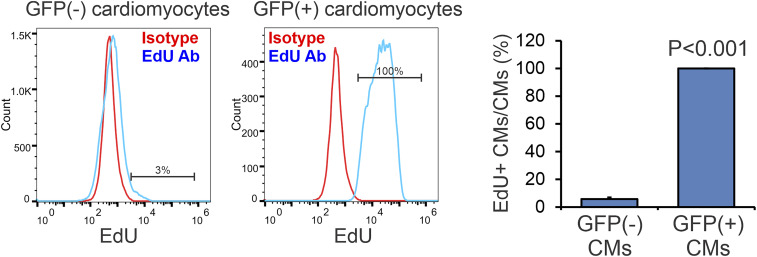
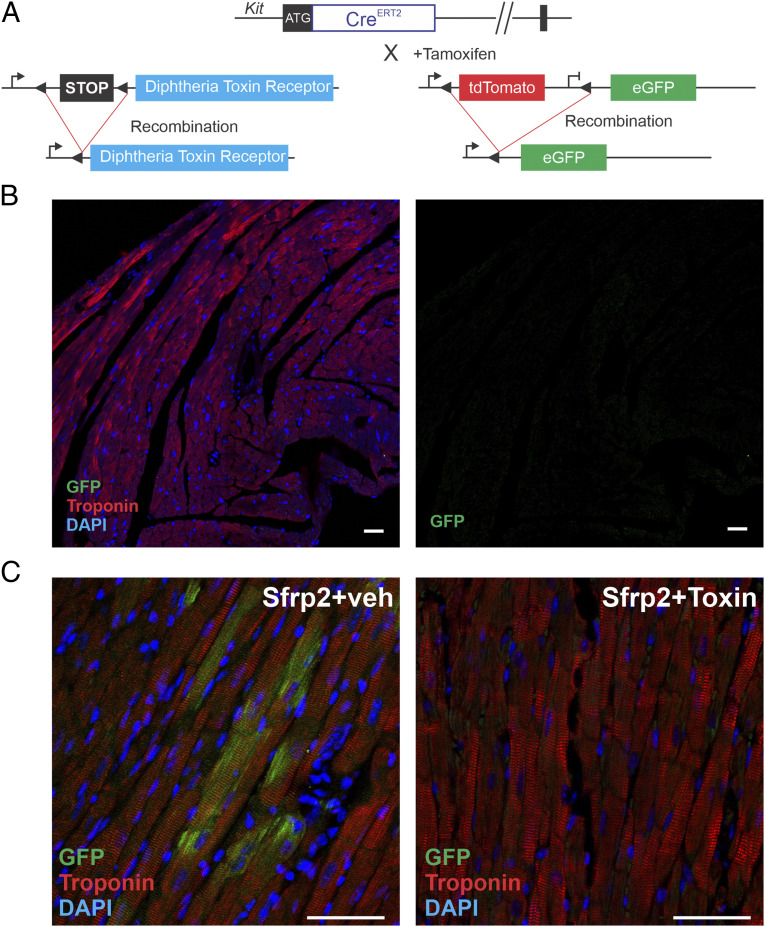
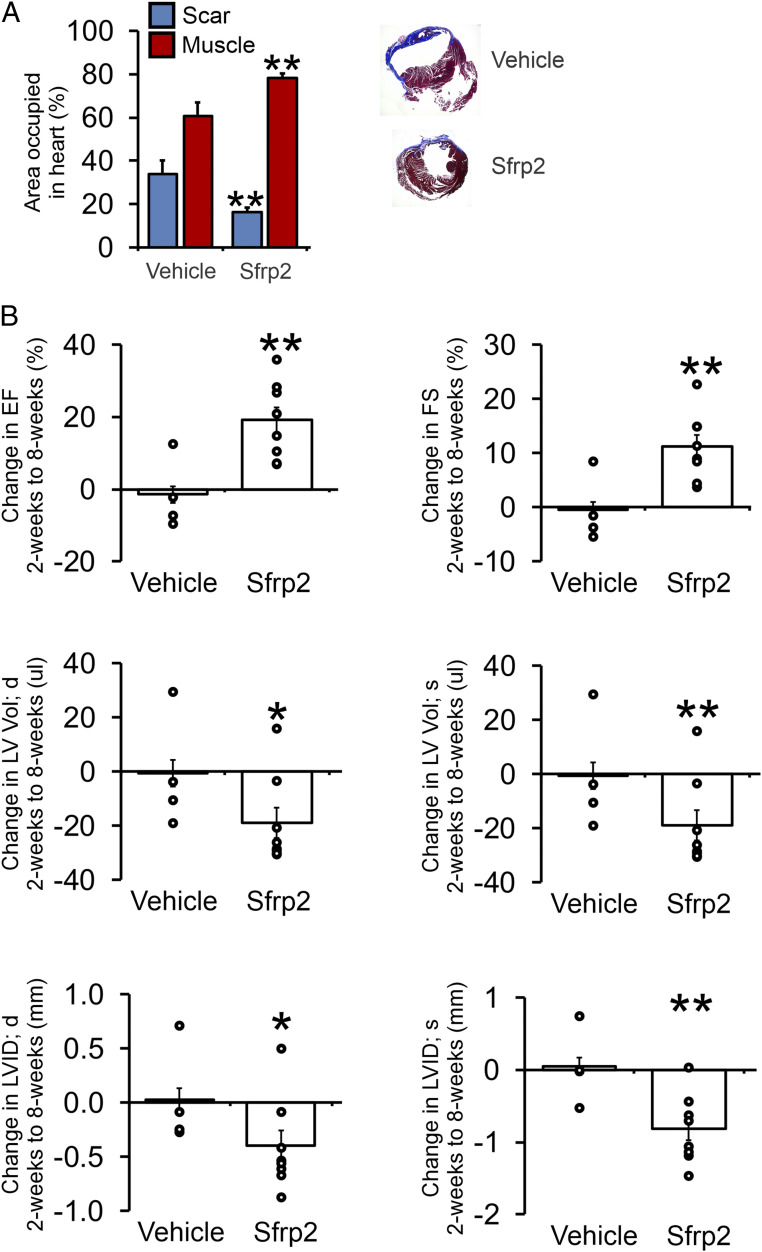
Cardiomyogenesis, the process by which the body generates cardiomyocytes, is poorly understood. We have recently shown that Sfrp2 promotes cardiomyogenesis in vitro. The objective of this study was to determine if Sfrp2 would similarly promote cardiomyogenesis in vivo. To test this hypothesis, we tracked multipotent cKit(+) cells in response to Sfrp2 treatment. In control adult mice, multipotent cKit(+) cells typically differentiated into endothelial cells but not cardiomyocytes. In contrast, Sfrp2 switched the fate of these cells. Following Sfrp2 injection, multipotent cKit(+) cells differentiated solely into cardiomyocytes. Sfrp2-derived cardiomyocytes integrated into the myocardium and exhibited identical physiological properties to preexisting native cardiomyocytes. The ability of Sfrp2 to promote cardiomyogenesis was further supported by tracking EdU-labeled cells. In addition, Sfrp2 did not promote the formation of new cardiomyocytes when the cKit(+) cell population was selectively ablated in vivo using a diphtheria toxin receptor-diphtheria toxin model. Notably, Sfrp2-induced cardiomyogenesis was associated with significant functional improvements in a cardiac injury model. In summary, our study further demonstrates the importance of Sfrp2 in cardiomyogenesis.
Keywords: Wnt signaling pathway; cell differentiation; cell lineage; heart injuries/pathology; myocytes.
Conflict of interest statement
The authors declare no competing interest.
Figures
References
-
- Jennings R. B., Reimer K. A., The cell biology of acute myocardial ischemia. Annu. Rev. Med. 42, 225–246 (1991). - PubMed
-
- Cleutjens J. P., Blankesteijn W. M., Daemen M. J., Smits J. F., The infarcted myocardium: Simply dead tissue, or a lively target for therapeutic interventions. Cardiovasc. Res. 44, 232–241 (1999). - PubMed
-
- Später D., Hansson E. M., Zangi L., Chien K. R., How to make a cardiomyocyte. Development 141, 4418–4431 (2014). - PubMed
-
- Jeziorowska D., Korniat A., Salem J. E., Fish K., Hulot J. S., Generating patient-specific induced pluripotent stem cells-derived cardiomyocytes for the treatment of cardiac diseases. Expert Opin. Biol. Ther. 15, 1399–1409 (2015). - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
