

Imaging of abdominal complications of COVID-19 infection
- PMID: 34381937
- PMCID: PMC8320136
- DOI: 10.1259/bjro.20200052
Imaging of abdominal complications of COVID-19 infection
Abstract
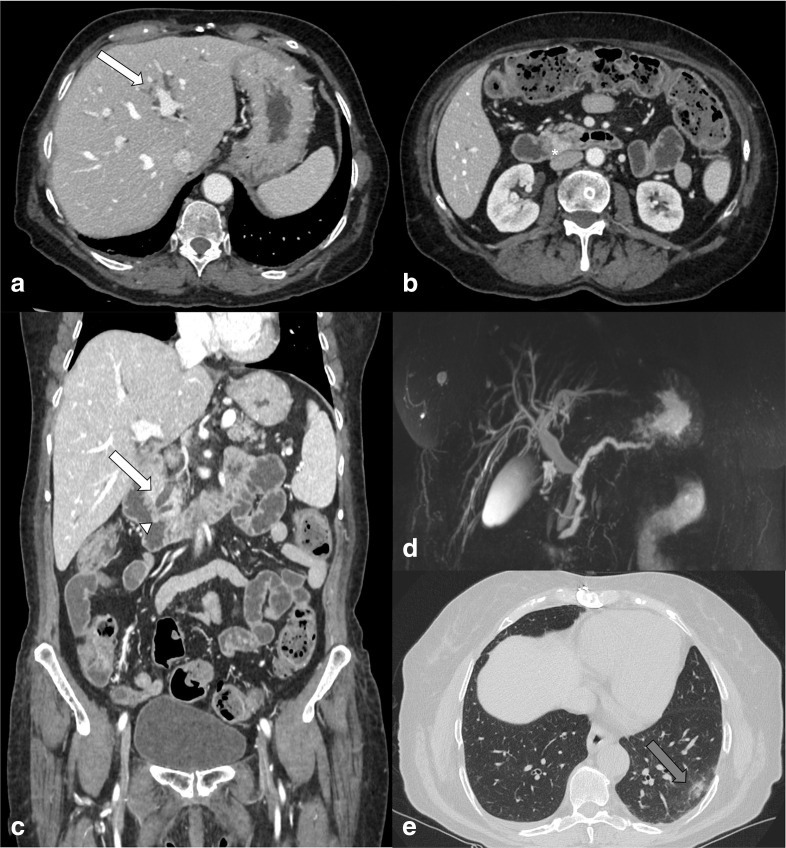
Coronavirus disease 2019 (COVID-19) is a respiratory syndrome caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) first described in Wuhan, Hubei Province, China in the last months of 2019 and then declared as a pandemic. Typical symptoms are represented by fever, cough, dyspnea and fatigue, but SARS-CoV-2 infection can also cause gastrointestinal symptoms (vomiting, diarrhoea, abdominal pain, loss of appetite) or be totally asymptomatic. As reported in literature, many patients with COVID-19 pneumonia had a secondary abdominal involvement (bowel, pancreas, gallbladder, spleen, liver, kidneys), confirmed by laboratory tests and also by radiological features. Usually the diagnosis of COVID-19 is suspected and then confirmed by real-time reverse-transcription-polymerase chain reaction (RT-PCR), after the examination of the lung bases of patients, admitted to the emergency department with abdominal symptoms and signs, who underwent abdominal-CT. The aim of this review is to describe the typical and atypical abdominal imaging findings in patients with SARS-CoV-2 infection reported since now in literature.
© 2021 The Authors. Published by the British Institute of Radiology.
Figures
Similar articles
-
Imaging and clinical features of patients with 2019 novel coronavirus SARS-CoV-2.Eur J Nucl Med Mol Imaging. 2020 May;47(5):1275-1280. doi: 10.1007/s00259-020-04735-9. Epub 2020 Feb 28. Eur J Nucl Med Mol Imaging. 2020. PMID: 32107577 Free PMC article.
-
Mining the Characteristics of COVID-19 Patients in China: Analysis of Social Media Posts.J Med Internet Res. 2020 May 17;22(5):e19087. doi: 10.2196/19087. J Med Internet Res. 2020. PMID: 32401210 Free PMC article.
-
Sars-Cov-19 associated with aspiration pneumonia in a patient with Parkinson disease: A case report.Eur J Radiol Open. 2021;8:100379. doi: 10.1016/j.ejro.2021.100379. Epub 2021 Oct 2. Eur J Radiol Open. 2021. PMID: 34632001 Free PMC article.
-
Gastrointestinal Infection Could Be New Focus for Coronavirus Diagnosis.Cureus. 2020 Mar 26;12(3):e7422. doi: 10.7759/cureus.7422. Cureus. 2020. PMID: 32351807 Free PMC article. Review.
-
Thoracic imaging tests for the diagnosis of COVID-19.Cochrane Database Syst Rev. 2020 Sep 30;9:CD013639. doi: 10.1002/14651858.CD013639.pub2. Cochrane Database Syst Rev. 2020. Update in: Cochrane Database Syst Rev. 2020 Nov 26;11:CD013639. doi: 10.1002/14651858.CD013639.pub3. PMID: 32997361 Updated.
Cited by
-
Extracorporeal membrane oxygenation (ECMO) in COVID-19 patients: a pocket guide for radiologists.Radiol Med. 2022 Apr;127(4):369-382. doi: 10.1007/s11547-022-01473-w. Epub 2022 Mar 13. Radiol Med. 2022. PMID: 35279765 Free PMC article. Review.
-
An Imaging Overview of COVID-19 ARDS in ICU Patients and Its Complications: A Pictorial Review.Diagnostics (Basel). 2022 Mar 29;12(4):846. doi: 10.3390/diagnostics12040846. Diagnostics (Basel). 2022. PMID: 35453894 Free PMC article. Review.
-
Ultrasound during the COVID-19 Pandemic: A Global Approach.J Clin Med. 2023 Jan 29;12(3):1057. doi: 10.3390/jcm12031057. J Clin Med. 2023. PMID: 36769702 Free PMC article. Review.
-
A Pictorial Essay Describing the CT Imaging Features of COVID-19 Cases throughout the Pandemic with a Special Focus on Lung Manifestations and Extrapulmonary Vascular Abdominal Complications.Biomedicines. 2023 Jul 26;11(8):2113. doi: 10.3390/biomedicines11082113. Biomedicines. 2023. PMID: 37626610 Free PMC article. Review.
-
Splenic infarction: an uncommon yet significant complication in COVID-19 patients - a case series report and literature review.Infez Med. 2023 Dec 1;31(4):560-569. doi: 10.53854/liim-3104-15. eCollection 2023. Infez Med. 2023. PMID: 38075427 Free PMC article.
References
-
- WHO . Coronavirus disease (COVID-19) pandemic 2020. 2020. Available from: https://www.who.int/emergencies/diseases/novel-coronavirus-2019.
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
