

Chronic low-grade inflammation in heart failure with preserved ejection fraction
- PMID: 34382743
- PMCID: PMC8441359
- DOI: 10.1111/acel.13453
Chronic low-grade inflammation in heart failure with preserved ejection fraction
Abstract
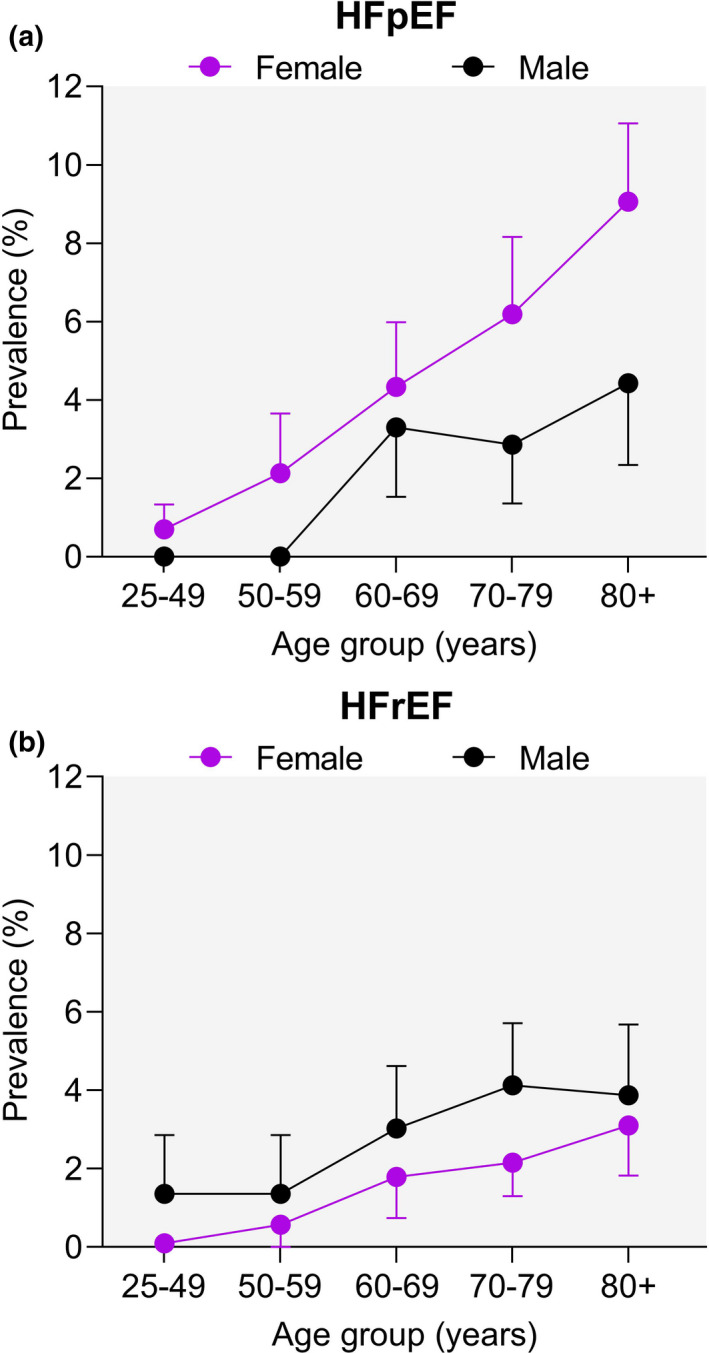
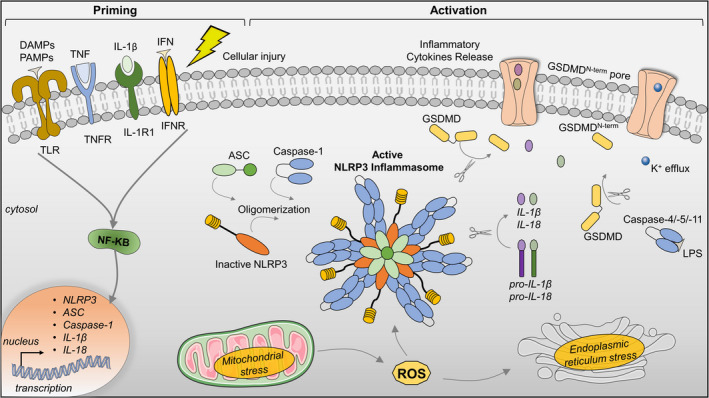
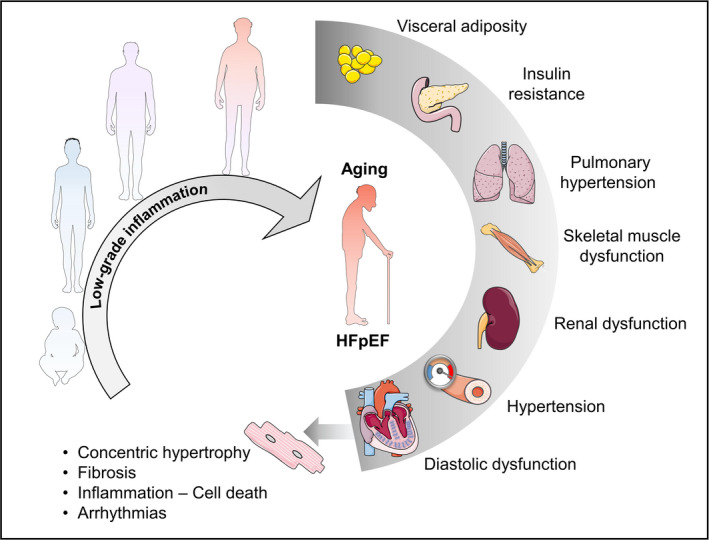
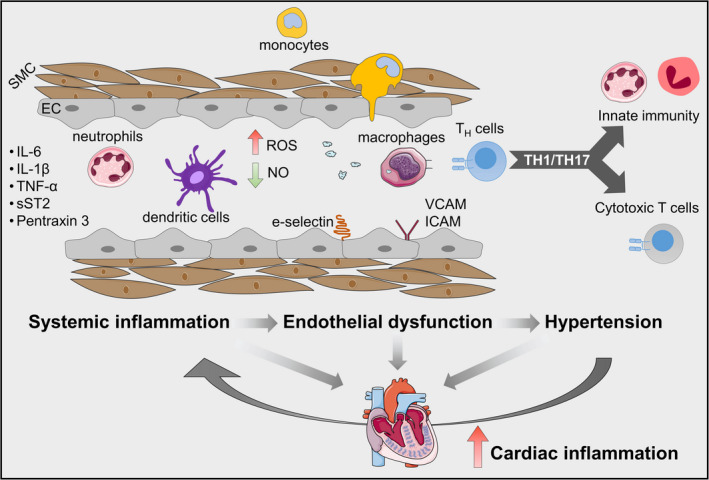
Heart failure (HF) with preserved ejection fraction (HFpEF) is currently the predominant form of HF with a dramatic increase in risk with age. Low-grade inflammation, as occurs with aging (termed "inflammaging"), is a common feature of HFpEF pathology. Suppression of proinflammatory pathways has been associated with attenuated HFpEF disease severity and better outcomes. From this perspective, inflammasome signaling plays a central role in mediating chronic inflammation and cardiovascular disease progression. However, the causal link between the inflammasome-immune signaling axis on the age-dependent progression of HFpEF remains conjectural. In this review, we summarize the current understanding of the role of inflammatory pathways in age-dependent cardiac function decline. We will also evaluate recent advances and evidence regarding the inflammatory pathway in the pathophysiology of HFpEF, with special attention to inflammasome signaling.
Keywords: aging; arrhythmias; diastolic dysfunction; fibrosis; heart failure with preserved ejection fraction; inflammasome; inflammation.
© 2021 The Authors. Aging Cell published by the Anatomical Society and John Wiley & Sons Ltd.
Conflict of interest statement
None declared.
Figures
Similar articles
-
Contributions of Inflammation to Cardiometabolic Heart Failure with Preserved Ejection Fraction.Annu Rev Pathol. 2025 Jan;20(1):143-167. doi: 10.1146/annurev-pathmechdis-111523-023405. Epub 2025 Jan 2. Annu Rev Pathol. 2025. PMID: 39357068 Review.
-
A novel paradigm for heart failure with preserved ejection fraction: comorbidities drive myocardial dysfunction and remodeling through coronary microvascular endothelial inflammation.J Am Coll Cardiol. 2013 Jul 23;62(4):263-71. doi: 10.1016/j.jacc.2013.02.092. Epub 2013 May 15. J Am Coll Cardiol. 2013. PMID: 23684677 Review.
-
Cardiac diastolic and autonomic dysfunction are aggravated by central chemoreflex activation in heart failure with preserved ejection fraction rats.J Physiol. 2017 Apr 15;595(8):2479-2495. doi: 10.1113/JP273558. Epub 2017 Mar 19. J Physiol. 2017. PMID: 28181258 Free PMC article.
-
Impaired systolic function by strain imaging in heart failure with preserved ejection fraction.J Am Coll Cardiol. 2014 Feb 11;63(5):447-56. doi: 10.1016/j.jacc.2013.09.052. Epub 2013 Oct 30. J Am Coll Cardiol. 2014. PMID: 24184245 Free PMC article. Clinical Trial.
-
Cellular and Molecular Differences between HFpEF and HFrEF: A Step Ahead in an Improved Pathological Understanding.Cells. 2020 Jan 18;9(1):242. doi: 10.3390/cells9010242. Cells. 2020. PMID: 31963679 Free PMC article. Review.
Cited by
-
Potential Mechanisms of Epicardial Adipose Tissue Influencing Heart Failure with Preserved Ejection Fraction.Rev Cardiovasc Med. 2024 Sep 3;25(9):311. doi: 10.31083/j.rcm2509311. eCollection 2024 Sep. Rev Cardiovasc Med. 2024. PMID: 39355598 Free PMC article. Review.
-
Sudden Death and Ventricular Arrhythmias in Heart Failure With Preserved Ejection Fraction.Korean Circ J. 2022 Apr;52(4):251-264. doi: 10.4070/kcj.2021.0420. Korean Circ J. 2022. PMID: 35388994 Free PMC article. Review.
-
Identification of ageing-associated gene signatures in heart failure with preserved ejection fraction by integrated bioinformatics analysis and machine learning.Genes Dis. 2024 Dec 3;12(4):101478. doi: 10.1016/j.gendis.2024.101478. eCollection 2025 Jul. Genes Dis. 2024. PMID: 40330147 Free PMC article.
-
The Atrioventricular Coupling in Heart Failure: Pathophysiological and Therapeutic Aspects.Rev Cardiovasc Med. 2024 May 14;25(5):169. doi: 10.31083/j.rcm2505169. eCollection 2024 May. Rev Cardiovasc Med. 2024. PMID: 39076484 Free PMC article. Review.
-
Skeletal muscle phenotypic switching in heart failure with preserved ejection fraction.Front Cardiovasc Med. 2022 Dec 1;9:1016452. doi: 10.3389/fcvm.2022.1016452. eCollection 2022. Front Cardiovasc Med. 2022. PMID: 36531739 Free PMC article.
References
-
- Abernethy, A., Raza, S., Sun, J. L., Anstrom, K. J., Tracy, R., Steiner, J., VanBuren, P., & LeWinter, M. M. (2018). Pro‐inflammatory biomarkers in stable versus acutely decompensated heart failure with preserved ejection fraction. Journal of the American Heart Association, 7, e007385. - PMC - PubMed
-
- Adamo, L., Rocha‐Resende, C., Prabhu, S. D., & Mann, D. L. (2020). Reappraising the role of inflammation in heart failure. Nature Reviews Cardiology, 17, 269–285. - PubMed
-
- Aghajanian, H., Kimura, T., Rurik, J. G., Hancock, A. S., Leibowitz, M. S., Li, L., Scholler, J., Monslow, J., Lo, A., Han, W., Wang, T., Bedi, K., Morley, M. P., Saldana, R. A. L., Bolar, N. A., McDaid, K., Assenmacher, C.‐A., Smith, C. L., Wirth, D., … Epstein, J. A. (2019). Targeting cardiac fibrosis with engineered T cells. Nature, 573, 430–433. - PMC - PubMed
-
- Ather, S., Chan, W., Bozkurt, B., Aguilar, D., Ramasubbu, K., Zachariah, A. A., Wehrens, X. H., & Deswal, A. (2012). Impact of noncardiac comorbidities on morbidity and mortality in a predominantly male population with heart failure and preserved versus reduced ejection fraction. Journal of the American College of Cardiology, 59, 998–1005. - PMC - PubMed
-
- Baker, P. J., Boucher, D., Bierschenk, D., Tebartz, C., Whitney, P. G., D'Silva, D. B., Tanzer, M. C., Monteleone, M., Robertson, A. A. B., Cooper, M. A., Alvarez‐Diaz, S., Herold, M. J., Bedoui, S., Schroder, K., & Masters, S. L. (2015). NLRP3 inflammasome activation downstream of cytoplasmic LPS recognition by both caspase‐4 and caspase‐5. European Journal of Immunology, 45, 2918–2926. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
