

Femtomolar SARS-CoV-2 Antigen Detection Using the Microbubbling Digital Assay with Smartphone Readout Enables Antigen Burden Quantitation and Tracking
- PMID: 34383886
- PMCID: PMC8436368
- DOI: 10.1093/clinchem/hvab158
Femtomolar SARS-CoV-2 Antigen Detection Using the Microbubbling Digital Assay with Smartphone Readout Enables Antigen Burden Quantitation and Tracking
Abstract
Background: High-sensitivity severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) antigen assays are desirable to mitigate false negative results. Limited data are available to quantify and track SARS-CoV-2 antigen burden in respiratory samples from different populations.
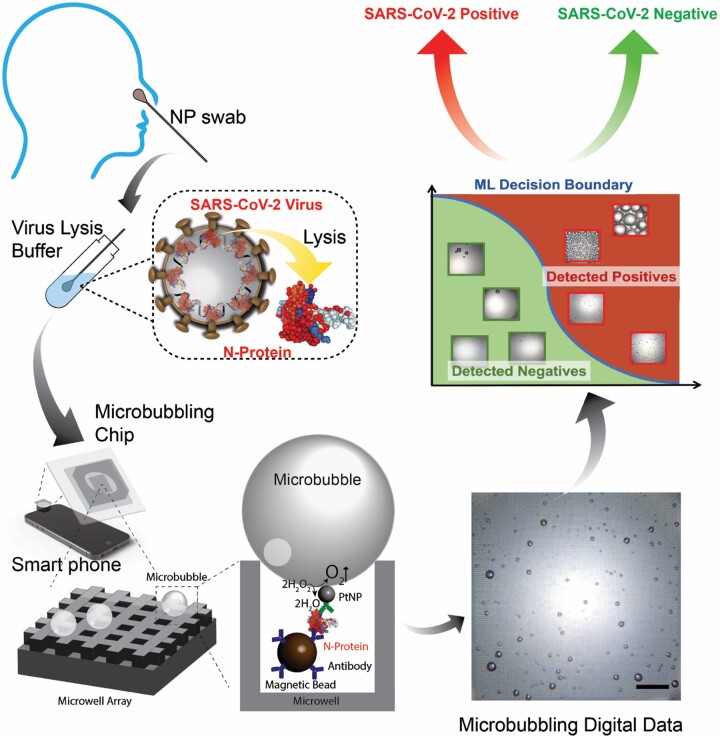
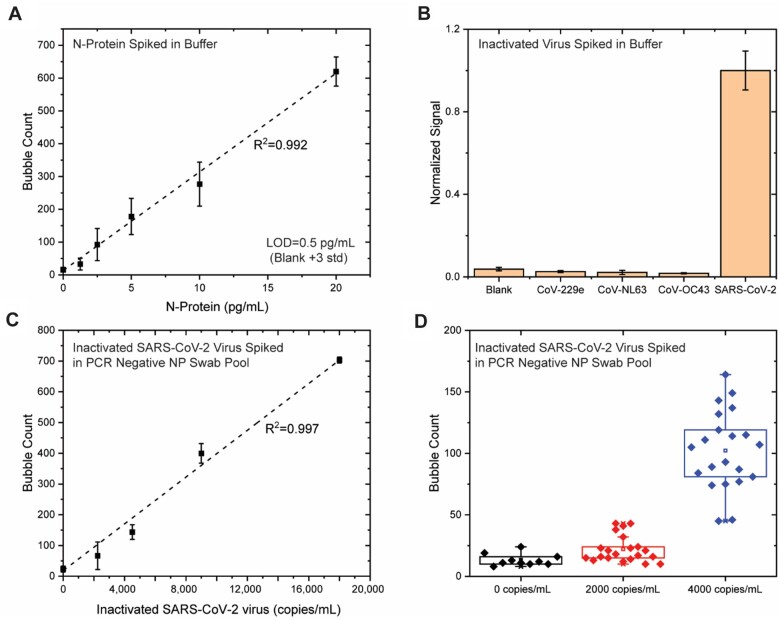
Methods: We developed the Microbubbling SARS-CoV-2 Antigen Assay (MSAA) with smartphone readout, with a limit of detection of 0.5 pg/mL (10.6 fmol/L) nucleocapsid antigen or 4000 copies/mL inactivated SARS-CoV-2 virus in nasopharyngeal (NP) swabs. We developed a computer vision and machine learning-based automatic microbubble image classifier to accurately identify positives and negatives and quantified and tracked antigen dynamics in intensive care unit coronavirus disease 2019 (COVID-19) inpatients and immunocompromised COVID-19 patients.
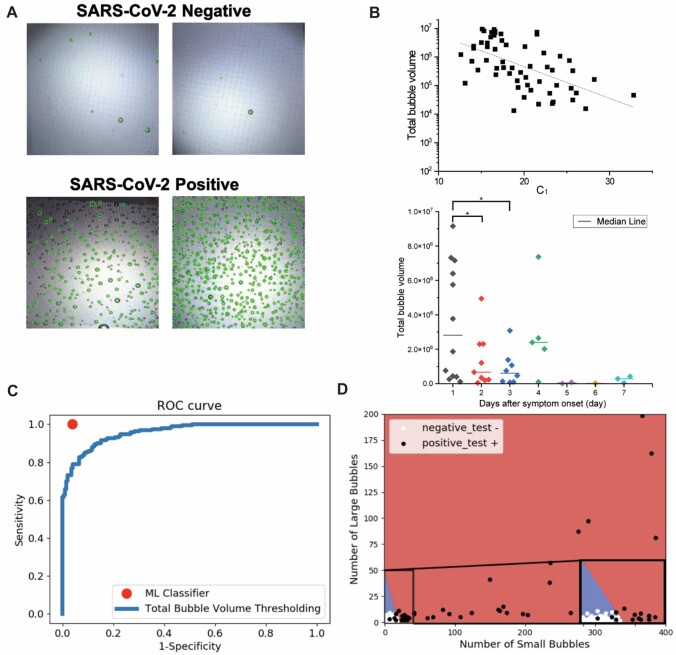
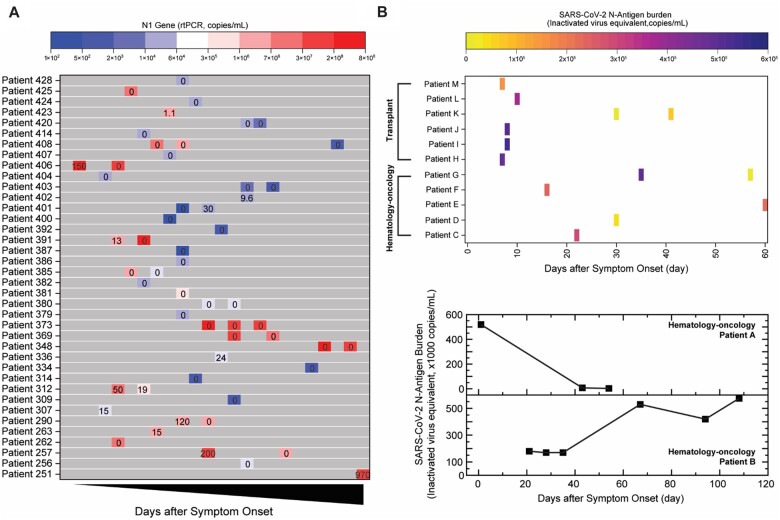
Results: Compared to qualitative reverse transcription-polymerase chain reaction methods, the MSAA demonstrated a positive percentage agreement of 97% (95% CI 92%-99%) and a negative percentage agreement of 97% (95% CI 94%-100%) in a clinical validation study with 372 residual clinical NP swabs. In immunocompetent individuals, the antigen positivity rate in swabs decreased as days-after-symptom-onset increased, despite persistent nucleic acid positivity. Antigen was detected for longer and variable periods of time in immunocompromised patients with hematologic malignancies. Total microbubble volume, a quantitative marker of antigen burden, correlated inversely with cycle threshold values and days-after-symptom-onset. Viral sequence variations were detected in patients with long duration of high antigen burden.
Conclusions: The MSAA enables sensitive and specific detection of acute infections and quantification and tracking of antigen burden and may serve as a screening method in longitudinal studies to identify patients who are likely experiencing active rounds of ongoing replication and warrant close viral sequence monitoring.
Keywords: SARS-CoV-2; longitudinal NP swab samples; microbubbling assay; viral antigen.
© American Association for Clinical Chemistry 2021. All rights reserved. For permissions, please email: journals.permissions@oup.com.
Figures
Update of
-
Femtomolar SARS-CoV-2 Antigen Detection Using the Microbubbling Digital Assay with Smartphone Readout Enables Antigen Burden Quantitation and Dynamics Tracking.medRxiv [Preprint]. 2021 Mar 26:2021.03.17.21253847. doi: 10.1101/2021.03.17.21253847. medRxiv. 2021. Update in: Clin Chem. 2021 Dec 30;68(1):230-239. doi: 10.1093/clinchem/hvab158. PMID: 33791710 Free PMC article. Updated. Preprint.
References
-
- SARS-CoV-2 reference panel comparative data. https://www.fda.gov/medical-devices/coronavirus-covid-19-and-medical-dev... (Accessed June 2021).
-
- Abbasi J. Researchers tie severe immunosuppression to chronic COVID-19 and virus variants. JAMA 2021;325:2033–5. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
