

Cannabigerolic acid, a major biosynthetic precursor molecule in cannabis, exhibits divergent effects on seizures in mouse models of epilepsy
- PMID: 34384142
- PMCID: PMC9292928
- DOI: 10.1111/bph.15661
Cannabigerolic acid, a major biosynthetic precursor molecule in cannabis, exhibits divergent effects on seizures in mouse models of epilepsy
Abstract
Background and purpose: Cannabis has been used to treat epilepsy for millennia, with such use validated by regulatory approval of cannabidiol (CBD) for Dravet syndrome. Unregulated artisanal cannabis-based products used to treat children with intractable epilepsies often contain relatively low doses of CBD but are enriched in other phytocannabinoids. This raises the possibility that other cannabis constituents might have anticonvulsant properties.
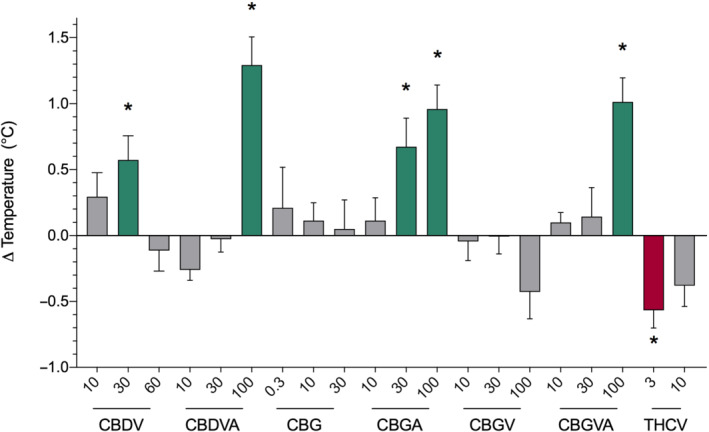
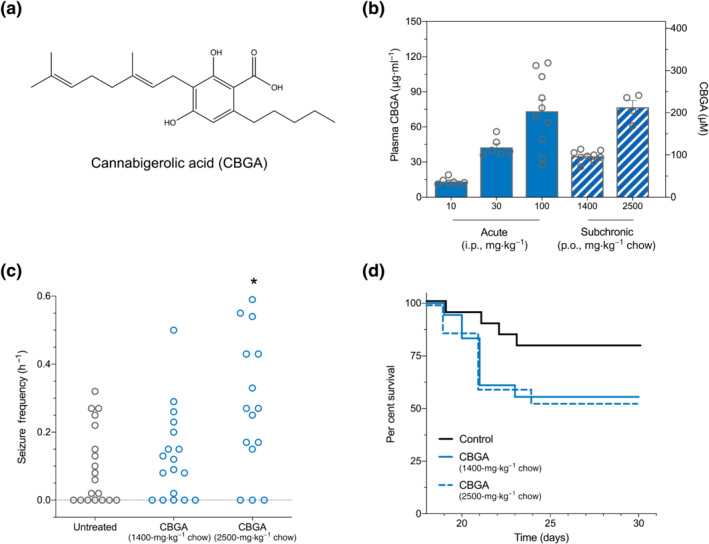
Experimental approach: We used the Scn1a+/- mouse model of Dravet syndrome to investigate the cannabis plant for phytocannabinoids with anticonvulsant effects against hyperthermia-induced seizures. The most promising, cannabigerolic acid (CBGA), was further examined against spontaneous seizures and survival in Scn1a+/- mice and in electroshock seizure models. Pharmacological effects of CBGA were surveyed across multiple drug targets.
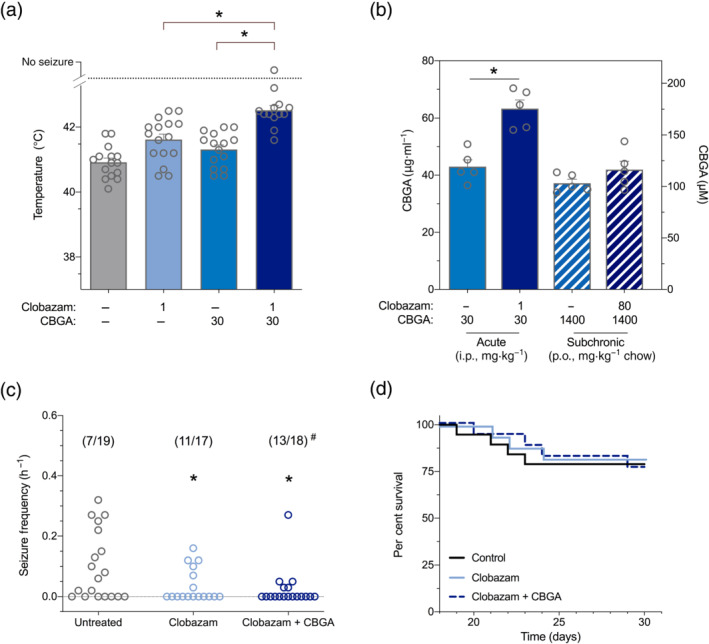
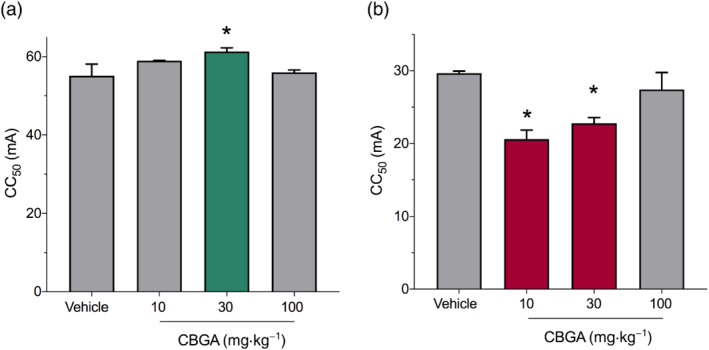
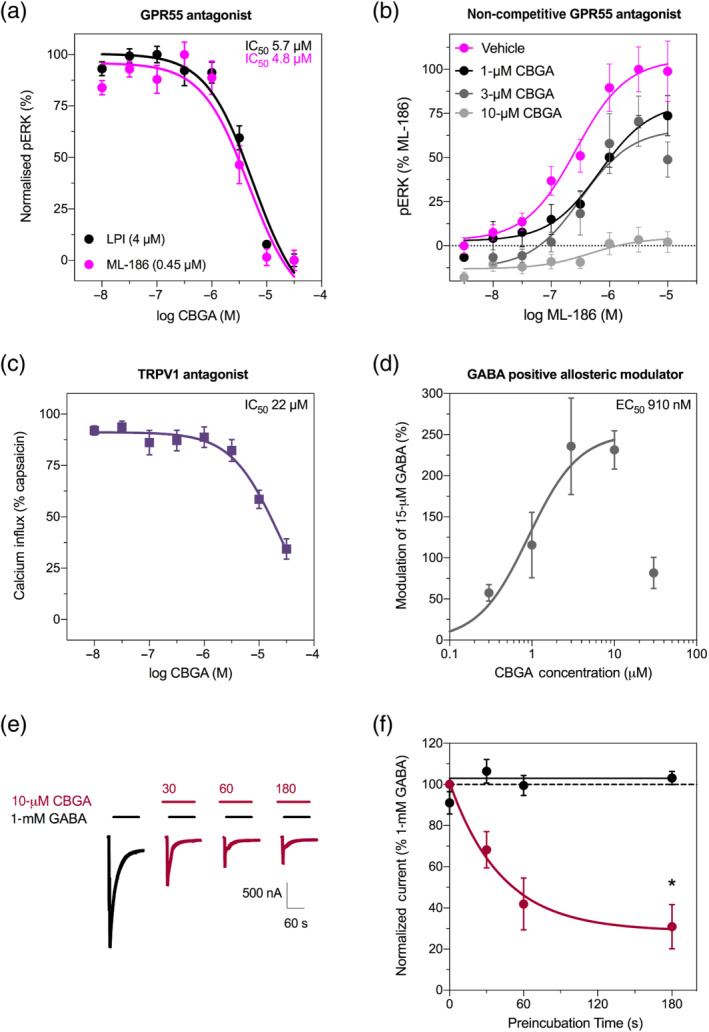
Key results: The initial screen identified three phytocannabinoids with novel anticonvulsant properties: CBGA, cannabidivarinic acid (CBDVA) and cannabigerovarinic acid (CBGVA). CBGA was most potent and potentiated the anticonvulsant effects of clobazam against hyperthermia-induced and spontaneous seizures, and was anticonvulsant in the MES threshold test. However, CBGA was proconvulsant in the 6-Hz threshold test and a high dose increased spontaneous seizure frequency in Scn1a+/- mice. CBGA was found to interact with numerous epilepsy-relevant targets including GPR55, TRPV1 channels and GABAA receptors.
Conclusion and implications: These results suggest that CBGA, CBDVA and CBGVA may contribute to the effects of cannabis-based products in childhood epilepsy. Although these phytocannabinoids have anticonvulsant potential and could be lead compounds for drug development programmes, several liabilities would need to be overcome before CBD is superseded by another in this class.
Keywords: CBGA; Dravet syndrome; cannabinoids; epilepsy.
© 2021 The Authors. British Journal of Pharmacology published by John Wiley & Sons Ltd on behalf of British Pharmacological Society.
Conflict of interest statement
J.C.A. has served as an expert witness in various medicolegal cases involving cannabis and cannabinoids and served as a temporary advisor to the World Health Organization (WHO) on their review of cannabis and the cannabinoids. I.S.M. is involved in an NHMRC‐funded clinical trial using the cannabis extract, nabiximols (Sativex®). He has served as an expert witness in various medicolegal cases involving cannabis and cannabinoids. J.C.A., L.L.A. and I.S.M. hold patents on cannabinoid therapies (PCT/AU2018/05089 and PCT/AU2019/050554). The remaining authors have no conflicts of interest.
Figures
References
-
- Absalom, N. L. , Ahring, P. K. , Liao, V. W. , Balle, T. , Jiang, T. , Anderson, L. L. , Arnold, J. C. , McGregor, I. S. , Bowen, M. T. , & Chebib, M. (2019). Functional genomics of epilepsy‐associated mutations in the GABAA receptor subunits reveal that one mutation impairs function and two are catastrophic. The Journal of Biological Chemistry, 294, 6157–6171. 10.1074/jbc.RA118.005697 - DOI - PMC - PubMed
-
- Alexander, S. P. H. , Christopoulos, A. , Davenport, A. P. , Kelly, E. , Mathie, A. , Peters, J. A. , Veale, E. L. , Armstrong, J. F. , Faccenda, E. , Harding, S. D. , Pawson, A. J. , Sharman, J. L. , Southan, C. , Davies, J. A. , Abbracchio, M. P. , Alexander, W. , Al‐hosaini, K. , Bäck, M. , Beaulieu, J. , … Yao, C. (2019). The Concise Guide to PHARMACOLOGY 2019/20: G protein‐coupled receptors. British Journal of Pharmacology, 176, S21–S141. 10.1111/bph.14748 - DOI - PMC - PubMed
-
- Anderson, L. L. , Absalom, N. L. , Abelev, S. V. , Low, I. K. , Doohan, P. T. , Martin, L. J. , Chebib, M. , McGregor, I. S. , & Arnold, J. C. (2019). Coadministered cannabidiol and clobazam: Preclinical evidence for both pharmacodynamic and pharmacokinetic interactions. Epilepsia, 60, 2224–2234. 10.1111/epi.16355 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
