

Resuscitative endovascular balloon occlusion of the aorta (REBOA) in patients with major trauma and uncontrolled haemorrhagic shock: a systematic review with meta-analysis
- PMID: 34384452
- PMCID: PMC8358549
- DOI: 10.1186/s13017-021-00386-9
Resuscitative endovascular balloon occlusion of the aorta (REBOA) in patients with major trauma and uncontrolled haemorrhagic shock: a systematic review with meta-analysis
Abstract
Background: Multiple studies regarding the use of Resuscitative Endovascular Balloon Occlusion of the Aorta (REBOA) in patients with non-compressible torso injuries and uncontrolled haemorrhagic shock were recently published. To date, the clinical evidence of the efficacy of REBOA is still debated. We aimed to conduct a systematic review assessing the clinical efficacy and safety of REBOA in patients with major trauma and uncontrolled haemorrhagic shock.
Methods: We systematically searched MEDLINE (PubMed), EMBASE and CENTRAL up to June 2020. All randomized controlled trials and observational studies that investigated the use of REBOA compared to resuscitative thoracotomy (RT) with/without REBOA or no-REBOA were eligible. We followed the PRISMA and MOOSE guidelines. Two authors independently extracted data and appraised the risk of bias of included studies. Effect sizes were pooled in a meta-analysis using random-effects models. The quality of evidence was assessed using the Grading of Recommendations Assessment, Development and Evaluation methodology. Primary outcomes were mortality, volume of infused blood components, health-related quality of life, time to haemorrhage control and any adverse effects. Secondary outcomes were improvement in haemodynamic status and failure/success of REBOA technique.
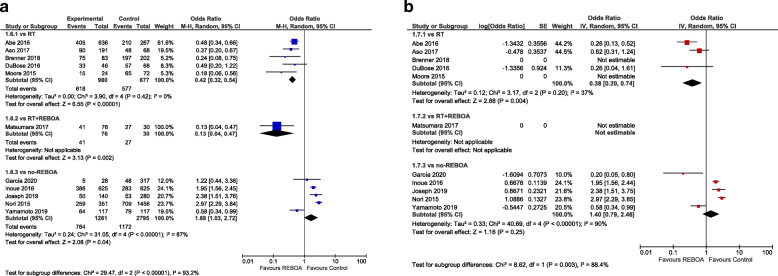
Results: We included 11 studies (5866 participants) ranging from fair to good quality. REBOA was associated with lower mortality when compared to RT (aOR 0.38; 95% CI 0.20-0.74), whereas no difference was observed when REBOA was compared to no-REBOA (aOR 1.40; 95% CI 0.79-2.46). No significant difference in health-related quality of life between REBOA and RT (p = 0.766). The most commonly reported complications were amputation, haematoma and pseudoaneurysm. Sparse data and heterogeneity of reporting for all other outcomes prevented any estimate.
Conclusions: Our findings on overall mortality suggest a positive effect of REBOA among non-compressible torso injuries when compared to RT but no differences compared to no-REBOA. Variability in indications and patient characteristics prevents any conclusion deserving further investigation. REBOA should be promoted in specific training programs in an experimental setting in order to test its effectiveness and a randomized trial should be planned.
Keywords: Systematic review, Resuscitative Endovascular Balloon Occlusion of the Aorta, Major trauma haemorrhage, Resuscitative thoracotomy.
© 2021. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- McGreevy DT, Sadeghi M, Pirouzram A, Toivola A, Dogan EM, Larzon T, et al. Feasibility and clinical outcome of Reboa in patients with impending traumatic cardiac arrest. Shock. 2019;16:1540–0514. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
