

Thoracic weighting of restrained subjects during exhaustion recovery causes loss of lung reserve volume in a model of police arrest
- PMID: 34385477
- PMCID: PMC8361138
- DOI: 10.1038/s41598-021-94157-w
Thoracic weighting of restrained subjects during exhaustion recovery causes loss of lung reserve volume in a model of police arrest
Abstract
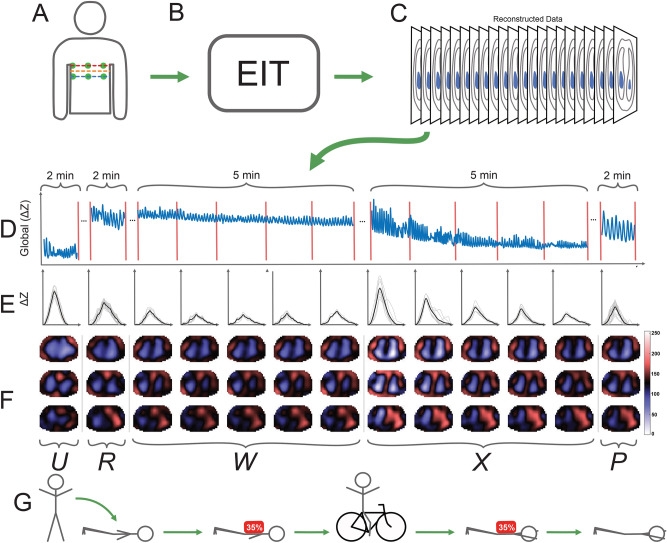
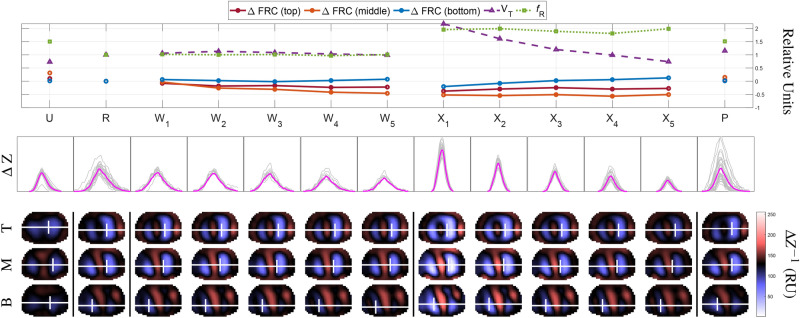
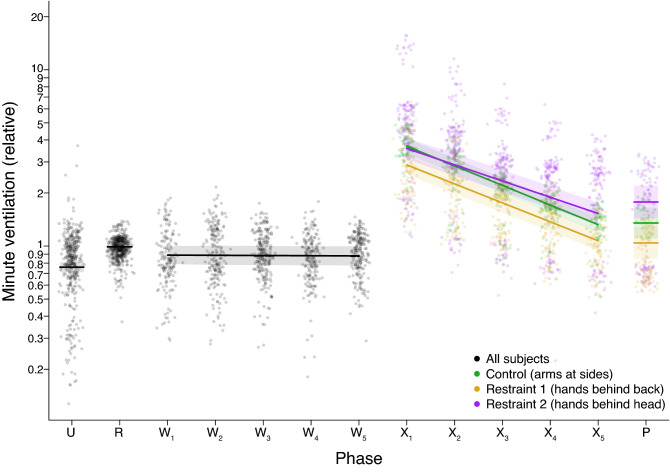
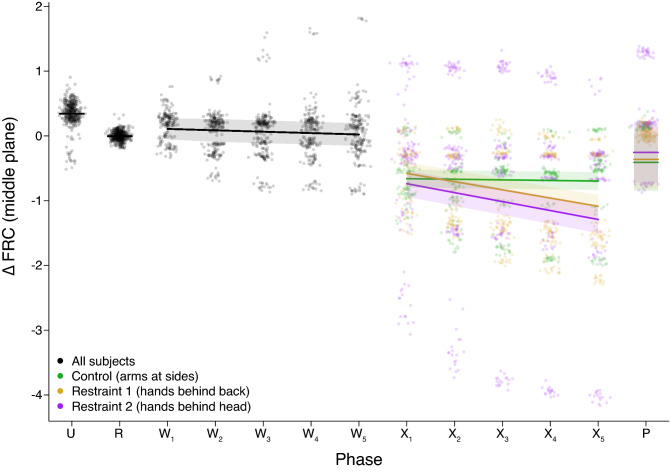
Restraint asphyxia has been proposed as a mechanism for some arrest-related deaths that occur during or shortly after a suspect is taken into custody. Our analysis of the literature found that prone positioning, weight applied to the back, recovery after simulated pursuit, and restraint position have led to restrictive, but non life-threatening respiratory changes when tested in subsets. However, the combined effects of all four parameters have not been tested together in a single study. We hypothesized that a complete protocol with high-sensitivity instrumentation could improve our understanding of breathing physiology during weighted restraint. We designed an electrical impedance tomography (EIT)-based protocol for this purpose and measured the 3D distribution of ventilation within the thorax. Here, we present the results from a study on 17 human subjects that revealed FRC declines during weighted restrained recovery from exercise for subjects in the restraint postures, but not the control posture. These prolonged FRC declines were consistent with abdominal muscle recruitment to assist the inspiratory muscles, suggesting that subjects in restraint postures have increased work of breathing compared to controls. Upon removal of the weighted load, lung reserve volumes gradually increased for the hands-behind-the-head restraint posture but continued to decrease for subjects in the hands-behind-the-back restraint posture. We discuss the possible role this increased work of breathing may play in restraint asphyxia.
© 2021. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Burch, A. Arrest-related deaths, 2003-2009—statistical tables. Tech. Rep. NCJ 235385, Bureau of Justice Statistics (2011).
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
