

Imaging of traumatic peripheral nerve injuries
- PMID: 34386344
- PMCID: PMC8333344
- DOI: 10.1016/j.jcot.2021.101510
Imaging of traumatic peripheral nerve injuries
Abstract
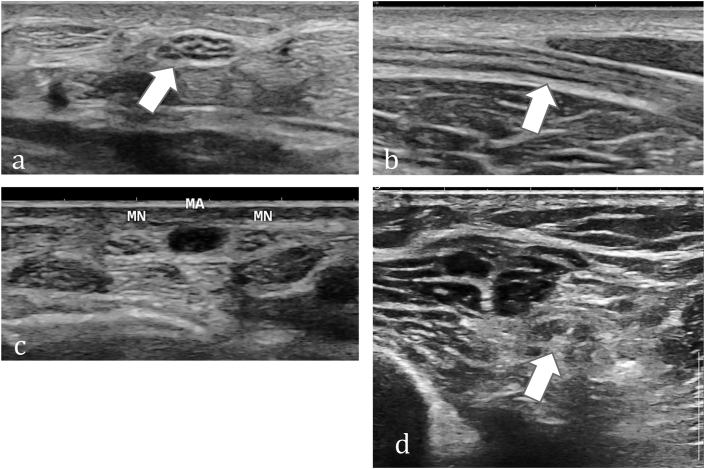
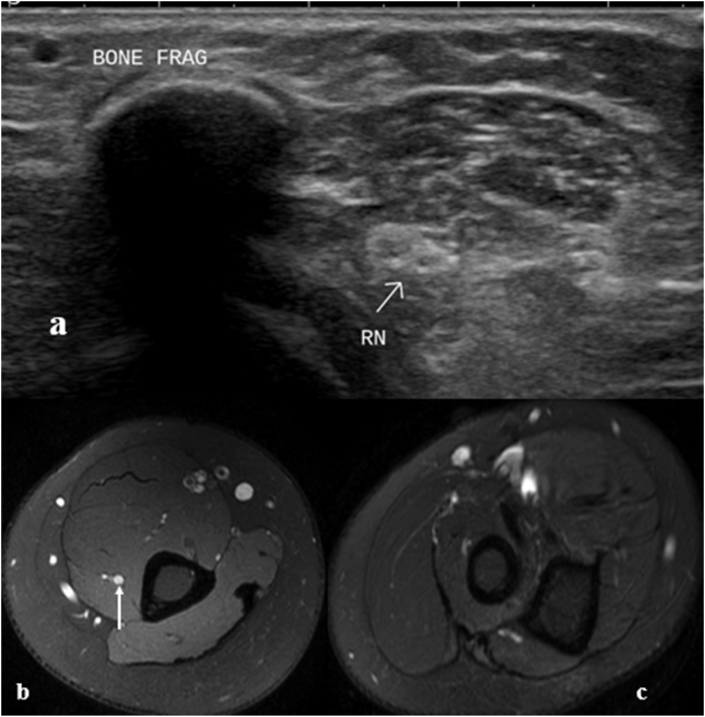
Nerves are commonly injured in case of blunt or penetrating trauma to the extremities. Patients with nerve injuries have profound consequences and thus a timely decision for operative management is a very important. Conventionally, management decisions have been based on clinical findings, patient course and electrophysiological studies. However, imaging modalities have an enormous role not only in localizing and grading of the nerve injuries but also in the follow-up of the nerve recovery. High-resolution ultrasound (HUS) is the modality of choice for evaluation of peripheral nerves. Magnetic resonance neurography (MRN) plays a complementary role, enabling better assessment of muscle changes and deeper nerves. Corresponding to the injured layer of the cross-section of the nerve, imaging manifestations differ in different grades of injury. Since imaging cannot detect ultrastructural changes at the microscopic level, thus there may be overlap in the imaging findings. Herewith, we discuss the imaging findings in different grades of nerve injury and propose a simple 3-tier grading for imaging (HUS and MRN) assessment of peripheral nerve injuries.
Keywords: High-resolution ultrasound (HUS); Magnetic resonance; Neurography (MRN); Peripheral nerve injuries.
© 2021 Delhi Orthopedic Association. All rights reserved.
Conflict of interest statement
The Authors declare that there is no conflict of interest.
Figures









Similar articles
-
Advanced Imaging of the Peripheral Nerves, From the AJR "How We Do It" Special Series.AJR Am J Roentgenol. 2024 Nov;223(5):e2430826. doi: 10.2214/AJR.24.30826. Epub 2024 Feb 14. AJR Am J Roentgenol. 2024. PMID: 38353448 Review.
-
Imaging of the Peripheral Nerve: Concepts and Future Direction of Magnetic Resonance Neurography and Ultrasound.J Hand Surg Am. 2019 Dec;44(12):1066-1079. doi: 10.1016/j.jhsa.2019.06.021. Epub 2019 Oct 2. J Hand Surg Am. 2019. PMID: 31585745 Review.
-
Magnetic resonance neurography of traumatic pediatric peripheral nerve injury: beyond birth-related brachial palsy.Pediatr Radiol. 2019 Jun;49(7):954-964. doi: 10.1007/s00247-019-04401-9. Epub 2019 May 11. Pediatr Radiol. 2019. PMID: 31079166 Review.
-
Magnetic resonance neurography for the evaluation of peripheral nerve, brachial plexus, and nerve root disorders.J Neurosurg. 2010 Feb;112(2):362-71. doi: 10.3171/2009.7.JNS09414. J Neurosurg. 2010. PMID: 19663545
-
Magnetic resonance neurography in the management of peripheral trigeminal neuropathy: experience in a tertiary care centre.Eur Radiol. 2016 Oct;26(10):3392-400. doi: 10.1007/s00330-015-4182-5. Epub 2016 Jan 21. Eur Radiol. 2016. PMID: 26795500
Cited by
-
Successful treatment of neurologic injury after complex spinal surgery with hyperbaric oxygen therapy: a case report.J Spine Surg. 2023 Jun 30;9(2):209-215. doi: 10.21037/jss-23-12. Epub 2023 May 24. J Spine Surg. 2023. PMID: 37435319 Free PMC article.
-
Sonographic evaluation of pediatric traumatic peripheral nerve injuries.Pediatr Radiol. 2025 Jul;55(8):1728-1740. doi: 10.1007/s00247-025-06253-y. Epub 2025 Jun 3. Pediatr Radiol. 2025. PMID: 40461879 Review.
-
Deep Learning-Based Knee MRI Classification for Common Peroneal Nerve Palsy with Foot Drop.Biomedicines. 2023 Nov 28;11(12):3171. doi: 10.3390/biomedicines11123171. Biomedicines. 2023. PMID: 38137392 Free PMC article.
-
The use of ultrasound-guided imaging to localize peripheral nerve injury in pediatric patients: A case report.Surg Neurol Int. 2024 Sep 27;15:347. doi: 10.25259/SNI_580_2024. eCollection 2024. Surg Neurol Int. 2024. PMID: 39372995 Free PMC article.
-
Ultrasound versus MR Neurography in Peripheral Nerve Diseases: Complimentary Rather than Competitive!Indian J Radiol Imaging. 2022 Aug 23;32(3):433-434. doi: 10.1055/s-0042-1754360. eCollection 2022 Sep. Indian J Radiol Imaging. 2022. PMID: 36177292 Free PMC article. No abstract available.
References
-
- Noble J., Munro C.A., Prasad V.S., Midha R. Analysis of upper and lower extremity peripheral nerve injuries in a population of patients with multiple injuries. J Trauma. 1998 Jul;45(1):116–122. - PubMed
-
- Smith P.J. Nerve injuries and their repair—a critical appraisal Sir Sydney Sunderland.560 pages, 158 illustrations. Churchill Livingstone, Edinburgh, 1991. ISBN 0–443–04161–X. Price £79.50. J Hand Surg. 1992;17(1):120–121.
-
- Friedman W.A. The electrophysiology of peripheral nerve injuries. Neurosurg Clin N Am. 1991;2(1):43–56. - PubMed
-
- Oh Sj M.D. first ed. Williams & Wilkins; Baltimore: 1998. Principles of Clinical Electromyography: Case Studies; p. 604.
LinkOut - more resources
Full Text Sources