

Study Designs to Assess Real-World Interventions to Prevent COVID-19
- PMID: 34386470
- PMCID: PMC8353119
- DOI: 10.3389/fpubh.2021.657976
Study Designs to Assess Real-World Interventions to Prevent COVID-19
Abstract
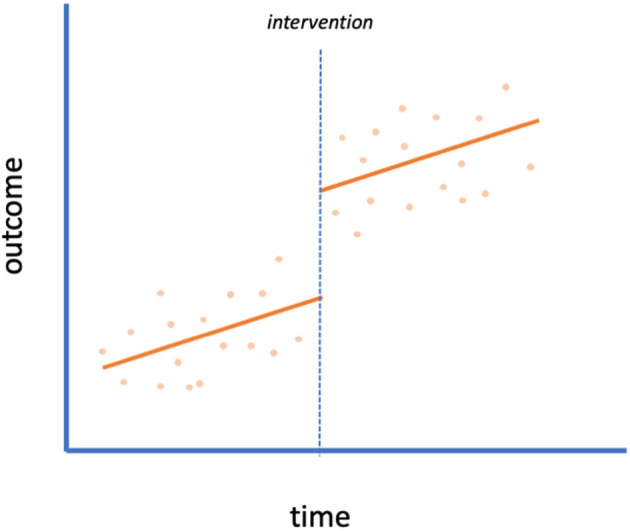
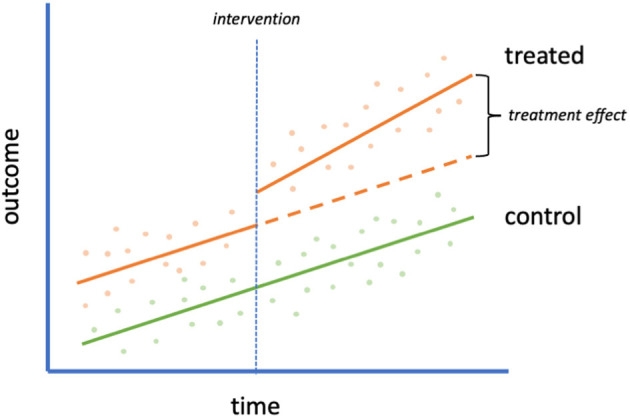
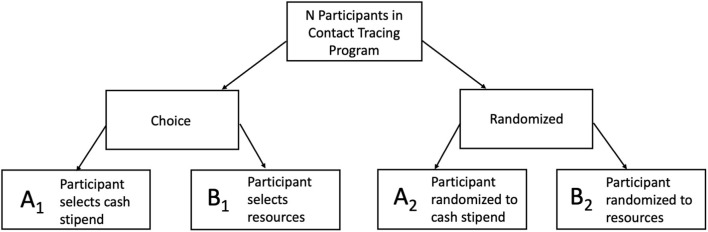
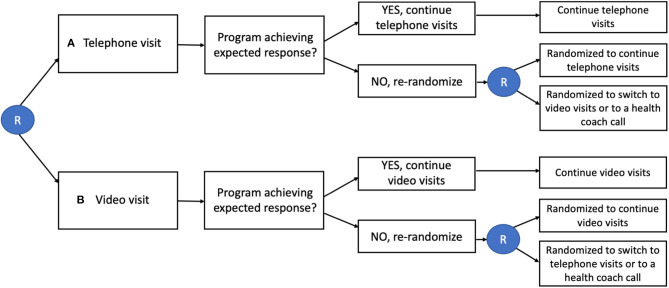
Background: In the face of the novel virus SARS-CoV-2, scientists and the public are eager for evidence about what measures are effective at slowing its spread and preventing morbidity and mortality. Other than mathematical modeling, studies thus far evaluating public health and behavioral interventions at scale have largely been observational and ecologic, focusing on aggregate summaries. Conclusions from these studies are susceptible to bias from threats to validity such as unmeasured confounding, concurrent policy changes, and trends over time. We offer recommendations on how to strengthen frequently applied study designs which have been used to understand the impact of interventions to reduce the spread of COVID-19, and suggest implementation-focused, pragmatic designs that, moving forward, could be used to build a robust evidence base for public health practice. Methods: We conducted a literature search of studies that evaluated the effectiveness of non-pharmaceutical interventions and policies to reduce spread, morbidity, and mortality of COVID-19. Our targeted review of the literature aimed to explore strengths and weaknesses of implemented studies, provide recommendations for improvement, and explore alternative real-world study design methods to enhance evidence-based decision-making. Results:Study designs such as pre/post, interrupted time series, and difference-in-differences have been used to evaluate policy effects at the state or country level of a range of interventions, such as shelter-in-place, face mask mandates, and school closures. Key challenges with these designs include the difficulty of disentangling the effects of contemporaneous changes in policy and correctly modeling infectious disease dynamics. Pragmatic study designs such as the SMART (Sequential, Multiple-Assignment Randomized Trial), stepped wedge, and preference designs could be used to evaluate community re-openings such as schools, and other policy changes. Conclusions: As the epidemic progresses, we need to move from post-hoc analyses of available data (appropriate for the beginning of the pandemic) to proactive evaluation to ensure the most rigorous approaches possible to evaluate the impact of COVID-19 prevention interventions. Pragmatic study designs, while requiring initial planning and community buy-in, could offer more robust evidence on what is effective and for whom to combat the global pandemic we face and future policy decisions.
Keywords: COVID-19; difference-in-differences; implementation science; interrupted time series; preference design; sequential multiple assignment randomized trial; stepped wedge; study design.
Copyright © 2021 Digitale, Stojanovski, McCulloch and Handley.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous