

A Pilot Study to Predict Risk of IgA Nephropathy Progression Based on miR-204 Expression
- PMID: 34386667
- PMCID: PMC8343780
- DOI: 10.1016/j.ekir.2021.05.018
A Pilot Study to Predict Risk of IgA Nephropathy Progression Based on miR-204 Expression
Abstract
Introduction: Immunoglobulin (Ig)A nephropathy (IgAN) is the most frequently diagnosed primary glomerulonephritis worldwide. Despite the common diagnostic feature of mesangial IgA-containing immune complex deposition, the clinical course of the disease is extremely variable, with 30% of patients developing end-stage kidney disease within 20 years of diagnosis. Therefore, identifying which patients are likely to progress is paramount.
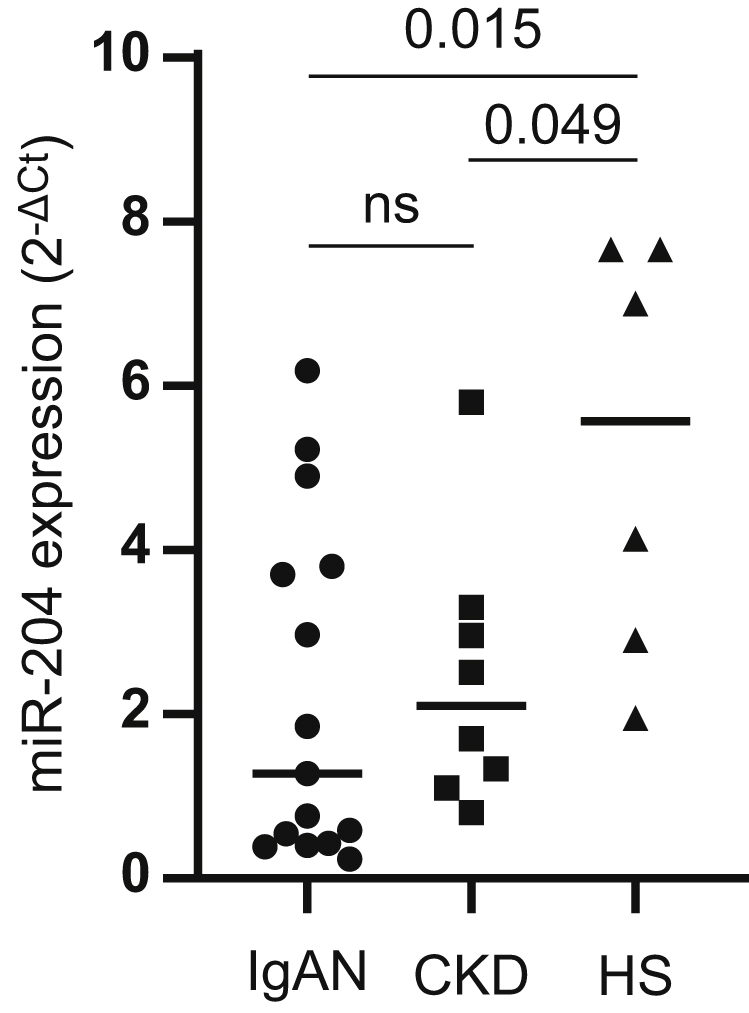
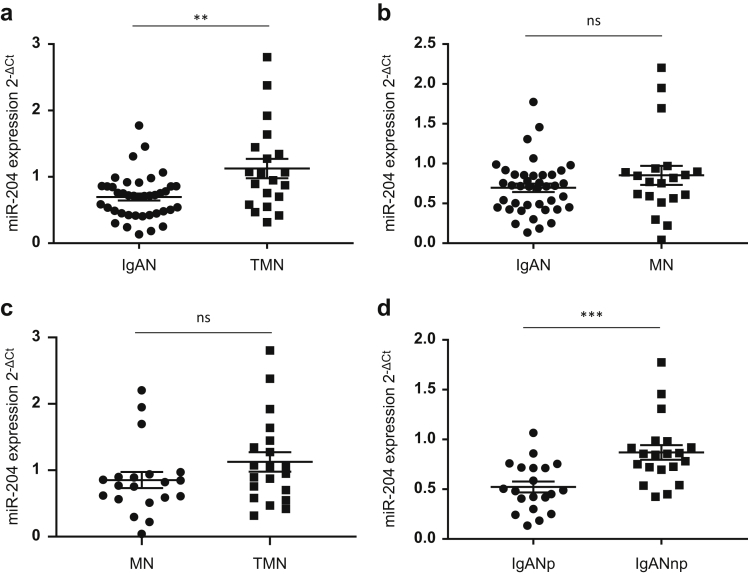
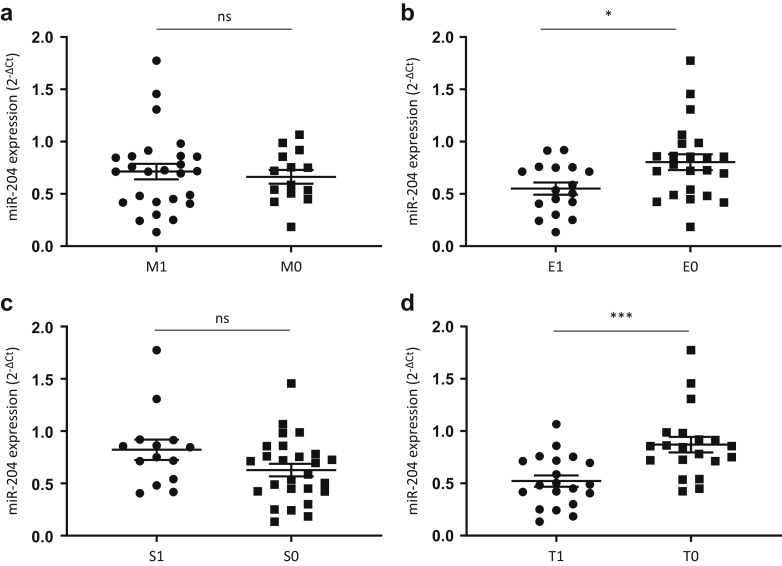
Results: In this pilot study, we found that urinary exosomal miR-204 expression was significantly reduced in IgAN compared with healthy subjects. However, there was no difference in miR-204 expression between IgAN and non-IgAN chronic kidney disease controls. Analysis of miR-204 expression in kidney biopsy cores by next-generation sequencing followed by quantitative polymerase chain reaction validation in independent cohorts demonstrated that expression of miR-204 was significantly lower in IgAN compared with thin-membrane nephropathy but not compared with membranous nephropathy. Patients with IgAN at high risk of future progression had significantly lower expression of miR-204 than those at low risk of progression. Cortical localization indicated that miR-204 was preferentially expressed in the interstitium compared with glomeruli in IgAN nonprogressors and that this distribution was lost in IgAN progressors. Receiver operating characteristic curve analysis between the 2 IgAN cohorts revealed an area under the curve of 0.82. In addition, miR-204 expression correlated with known clinicopathological prognostic risk factors. Importantly, incorporating miR-204 into the International IgAN risk prediction tool improved the diagnostic power of the algorithm to predict risk of progression.
Conclusion: Additional large-scale studies are now needed to validate the additive value of miR-204 in improving risk prediction in IgAN and more broadly in chronic kidney disease.
Keywords: IgA nephropathy; exosomes; microRNA; renal biopsy; renal progression.
© 2021 International Society of Nephrology. Published by Elsevier Inc.
Figures





References
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
Miscellaneous
