

Outcomes of respiratory viral-bacterial co-infection in adult hospitalized patients
- PMID: 34386745
- PMCID: PMC8343259
- DOI: 10.1016/j.eclinm.2021.100955
Outcomes of respiratory viral-bacterial co-infection in adult hospitalized patients
Abstract
Background: Viral infections of the respiratory tract represent a major global health concern. Co-infection with bacteria may contribute to severe disease and increased mortality in patients. Nevertheless, viral-bacterial co-infection patterns and their clinical outcomes have not been well characterized to date. This study aimed to evaluate the clinical features and outcomes of patients with viral-bacterial respiratory tract co-infections.
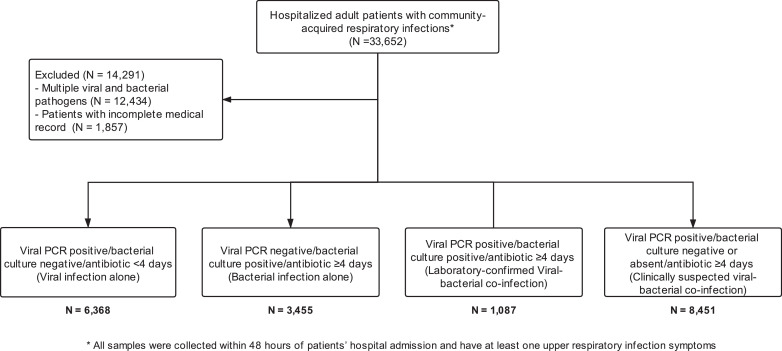
Methods: We included 19,361 patients with respiratory infection due to respiratory viruses [influenza A and B, respiratory syncytial virus (RSV), parainfluenza] and/or bacteria in four tertiary hospitals in Hong Kong from 2013 to 2017 using a large territory-wide healthcare database. All microbiological tests were conducted within 48 h of hospital admission. Four etiological groups were included: (1) viral infection alone; (2) bacterial infection alone; (3) laboratory-confirmed viral-bacterial co-infection and (4) clinically suspected viral-bacterial co-infection who were tested positive for respiratory virus and negative for bacteria but had received at least four days of antibiotics. Clinical features and outcomes were recorded for laboratory-confirmed viral-bacterial co-infection patients compared to other three groups as control. The primary outcome was 30-day mortality. Secondary outcomes were intensive care unit (ICU) admission and length of hospital stay. Propensity score matching estimated by binary logistic regression was used to adjust for the potential bias that may affect the association between outcomes and covariates.
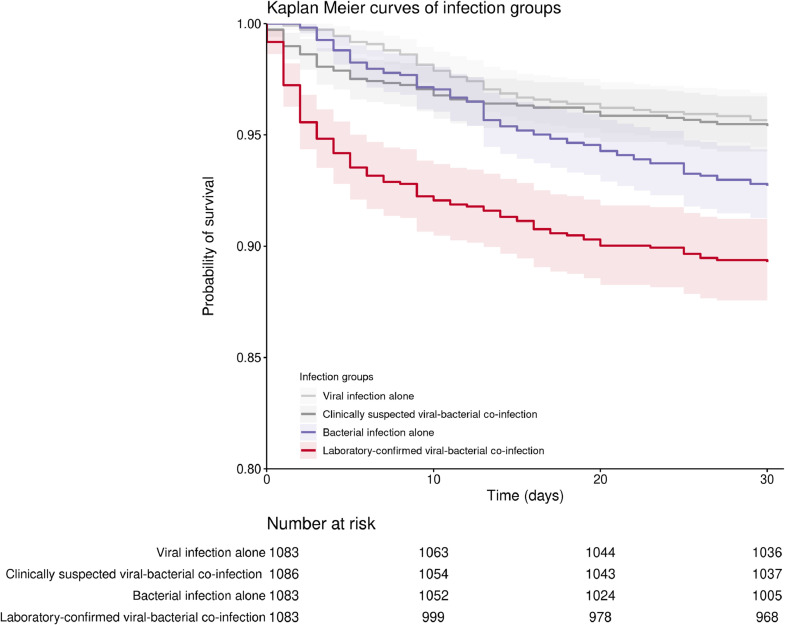
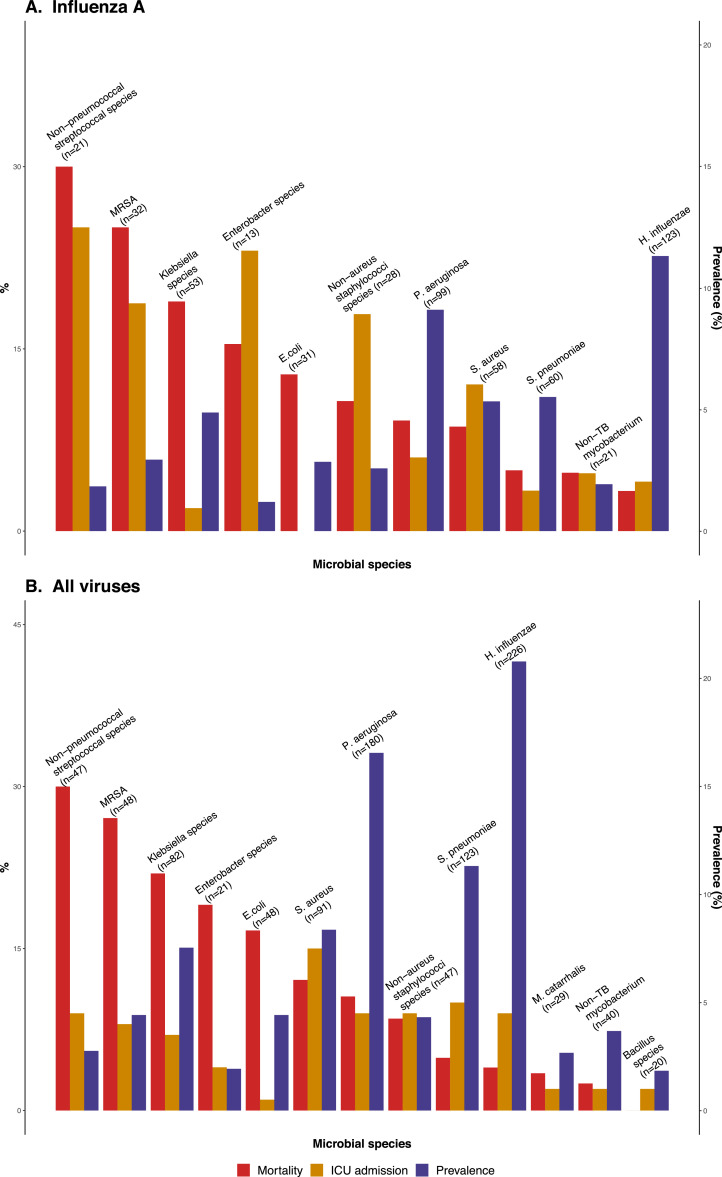
Findings: Among 15,906 patients with respiratory viral infection, there were 8451 (53.1%) clinically suspected and 1,087 (6.8%) laboratory-confirmed viral-bacterial co-infection. Among all the bacterial species, Haemophilus influenzae (226/1,087, 20.8%), Pseudomonas aeruginosa (180/1087, 16.6%) and Streptococcus pneumoniae (123/1087, 11.3%) were the three most common bacterial pathogens in the laboratory-confirmed co-infection group. Respiratory viruses co-infected with non-pneumococcal streptococci or methicillin-resistant Staphylococcus aureus was associated with the highest death rate [9/30 (30%) and 13/48 (27.1%), respectively] in this cohort. Compared with other infection groups, patients with laboratory-confirmed co-infection had higher ICU admission rate (p < 0.001) and mortality rate at 30 days (p = 0.028), and these results persisted after adjustment for potential confounders using propensity score matching. Furthermore, patients with laboratory-confirmed co-infection had significantly higher mortality compared to patients with bacterial infection alone.
Interpretation: In our cohort, bacterial co-infection is common in hospitalized patients with viral respiratory tract infection and is associated with higher ICU admission rate and mortality. Therefore, active surveillance for bacterial co-infection and early antibiotic treatment may be required to improve outcomes in patients with respiratory viral infection.
Keywords: Mortality; Respiratory; viral-bacterial co-infection.
© 2021 The Author(s).
Conflict of interest statement
Lowell Ling has received consulting fees from Merck Sharp & Dohme. Other authors declared that they have no conflict of interest.
Figures
References
-
- Bulla A., Hitze K.L. Acute respiratory infections: a review. Bull World Health Organ. 1978;56(3):481–498. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2395579/ - PMC - PubMed
-
- Millett E.R.C., Quint J.K., Smeeth L., Daniel R.M., Thomas S.L. Incidence of community-acquired lower respiratory tract infections and pneumonia among older adults in the united kingdom: a population-based study. PLoS ONE. 2013;8(9):e75131. doi: 10.1371/journal.pone.0075131. https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0075131 - DOI - PMC - PubMed
-
- Garibaldi R.A. Epidemiology of community-acquired respiratory tract infections in adults: incidence, etiology, and impact. Am J Med. 1985;78(6):32–37. doi: 10.1016/0002-9343(85)90361-4. http://www.sciencedirect.com/science/article/pii/0002934385903614 Supplement 2. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
