

What's behind 68Ga-PSMA-11 uptake in primary prostate cancer PET? Investigation of histopathological parameters and immunohistochemical PSMA expression patterns
- PMID: 34386839
- PMCID: PMC8484204
- DOI: 10.1007/s00259-021-05501-1
What's behind 68Ga-PSMA-11 uptake in primary prostate cancer PET? Investigation of histopathological parameters and immunohistochemical PSMA expression patterns
Abstract
Purpose: Prostate-specific membrane antigen (PSMA-) PET has become a promising tool in staging and restaging of prostate carcinoma (PCa). However, specific primary tumour features might impact accuracy of PSMA-PET for PCa detection. We investigated histopathological parameters and immunohistochemical PSMA expression patterns on radical prostatectomy (RPE) specimens and correlated them to the corresponding 68Ga-PSMA-11-PET examinations.
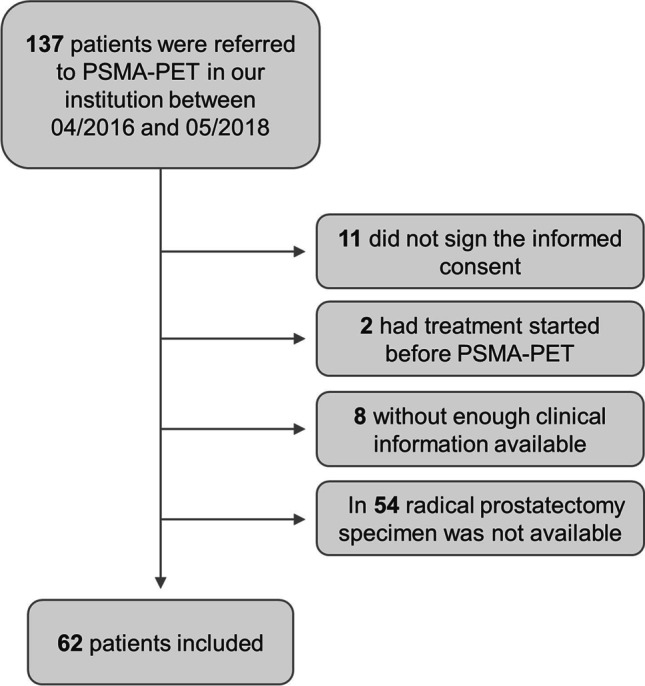
Methods: RPE specimens of 62 patients with preoperative 68Ga-PSMA-11-PET between 2016 and 2018 were analysed. WHO/ISUP grade groups, growth pattern (expansive vs. infiltrative), tumour area and diameter as well as immunohistochemical PSMA heterogeneity, intensity and negative tumour area (PSMA%neg) were correlated with spatially corresponding SUVmax on 68Ga-PSMA-11-PET in a multidisciplinary analysis.
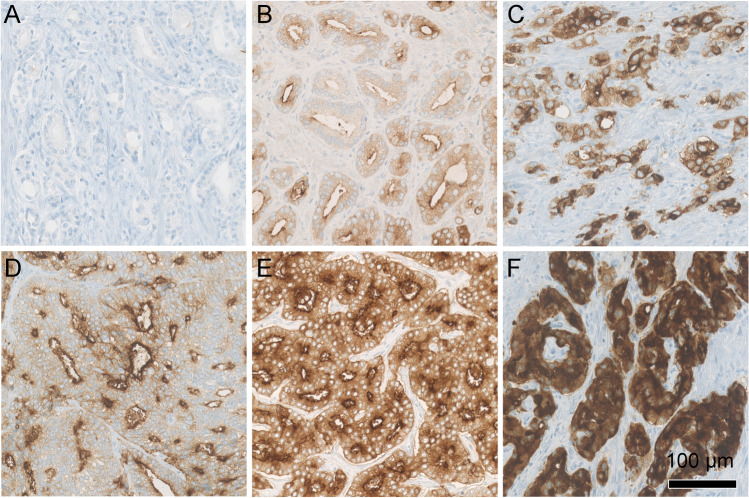
Results: All tumours showed medium to strong membranous (2-3 +) and weak to strong cytoplasmic (1-3 +) PSMA expression. Heterogeneously expressed PSMA was found in 38 cases (61%). Twenty-five cases (40%) showed at least 5% and up to 80% PSMA%neg. PSMA%neg, infiltrative growth pattern, smaller tumour area and diameter and WHO/ISUP grade group 2 significantly correlated with lower SUVmax values. A ROC curve analysis revealed 20% PSMA%neg as an optimal cutoff with the highest sensitivity and specificity (89% and 86%, AUC 0.923) for a negative PSMA-PET scan. A multiple logistic regression model revealed tumoural PSMA%neg (p < 0.01, OR = 9.629) and growth pattern (p = 0.0497, OR = 306.537) as significant predictors for a negative PSMA-PET scan.
Conclusions: We describe PSMA%neg, infiltrative growth pattern, smaller tumour size and WHO/ISUP grade group 2 as parameters associated with a lower 68Ga-PSMA-11 uptake in prostate cancer. These findings can serve as fundament for future biopsy-based biomarker development to enable an individualized, tumour-adapted imaging approach.
Keywords: Glutamate carboxypeptidase II; Immunohistochemistry; Neoplasm staging; Positron emission tomography; Prostatic neoplasms.
© 2021. The Author(s).
Conflict of interest statement
IAB has received research grants and speaker honorarium from GE Healthcare, research grants from Swiss Life and speaker honorarium from Bayer Health Care and Astellas Pharma AG.
TH holds an advisory function for MSD and Bayer.
NJR discloses an advisory board function and receipt of honoraria from F. Hoffmann-La Roche AG.
JHR, DAF, UJM, RL, AKR, HM and DE declare no conflict of interest.
The Department of Nuclear Medicine holds an institutional Research Contract with GE Healthcare.
Figures





References
-
- Mhawech-Fauceglia P, Zhang S, Terracciano L, Sauter G, Chadhuri A, Herrmann FR, et al. Prostate-specific membrane antigen (PSMA) protein expression in normal and neoplastic tissues and its sensitivity and specificity in prostate adenocarcinoma: an immunohistochemical study using mutiple tumour tissue microarray technique. Histopathology. 2007;50(4):472–483. doi: 10.1111/j.1365-2559.2007.02635.x. - DOI - PubMed
-
- Ross JS, Sheehan CE, Fisher HA, Kaufman RP, Jr, Kaur P, Gray K, et al. Correlation of primary tumor prostate-specific membrane antigen expression with disease recurrence in prostate cancer. Clin Cancer Res. 2003;9(17):6357–6362. - PubMed
-
- Hupe MC, Philippi C, Roth D, Kumpers C, Ribbat-Idel J, Becker F, et al. Expression of prostate-specific membrane antigen (PSMA) on biopsies is an independent risk stratifier of prostate cancer patients at time of initial diagnosis. Front Oncol. 2018;8:623. doi: 10.3389/fonc.2018.00623. - DOI - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
