

Comparative Effectiveness of Implantable Defibrillators for Asymptomatic Brugada Syndrome: A Decision-Analytic Model
- PMID: 34387130
- PMCID: PMC8475040
- DOI: 10.1161/JAHA.121.021144
Comparative Effectiveness of Implantable Defibrillators for Asymptomatic Brugada Syndrome: A Decision-Analytic Model
Abstract
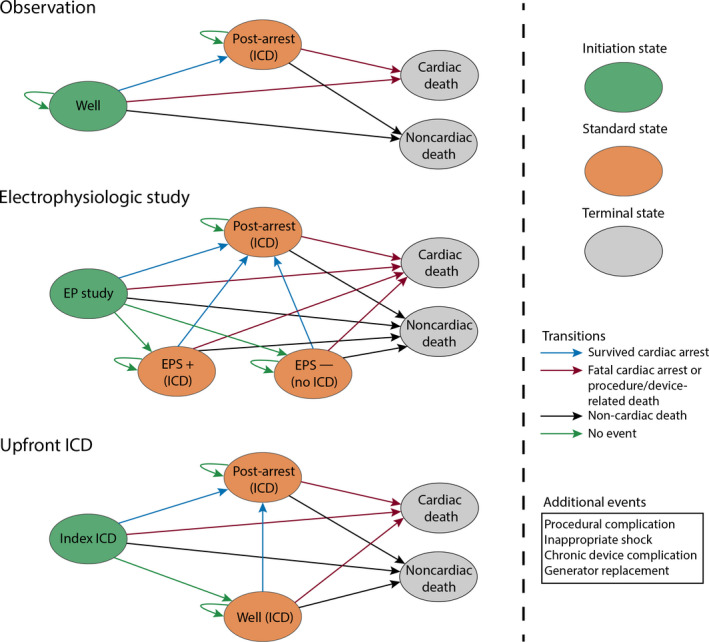
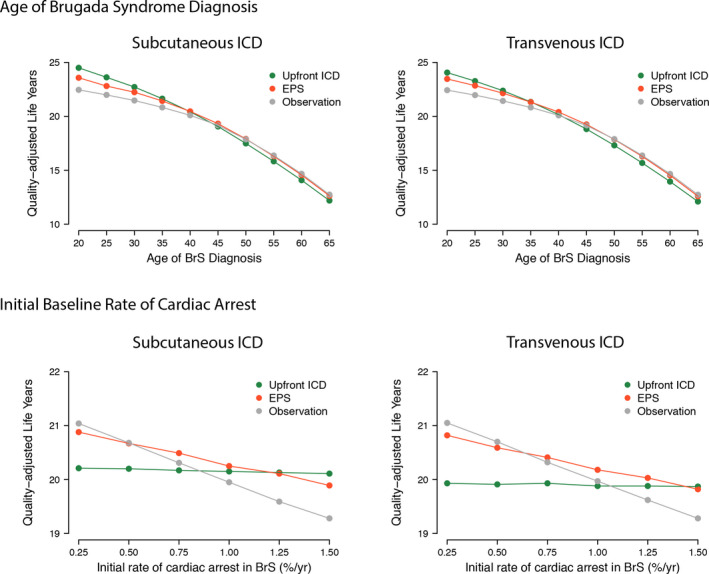
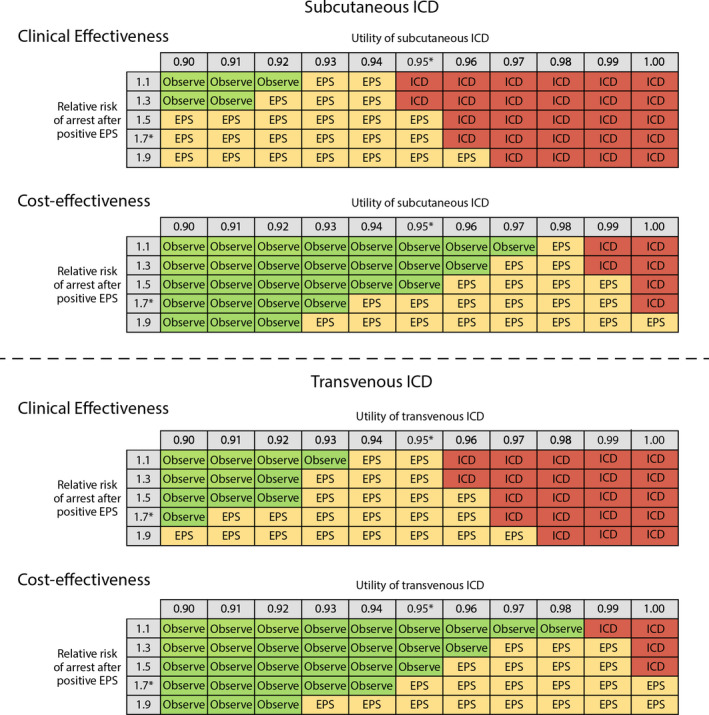
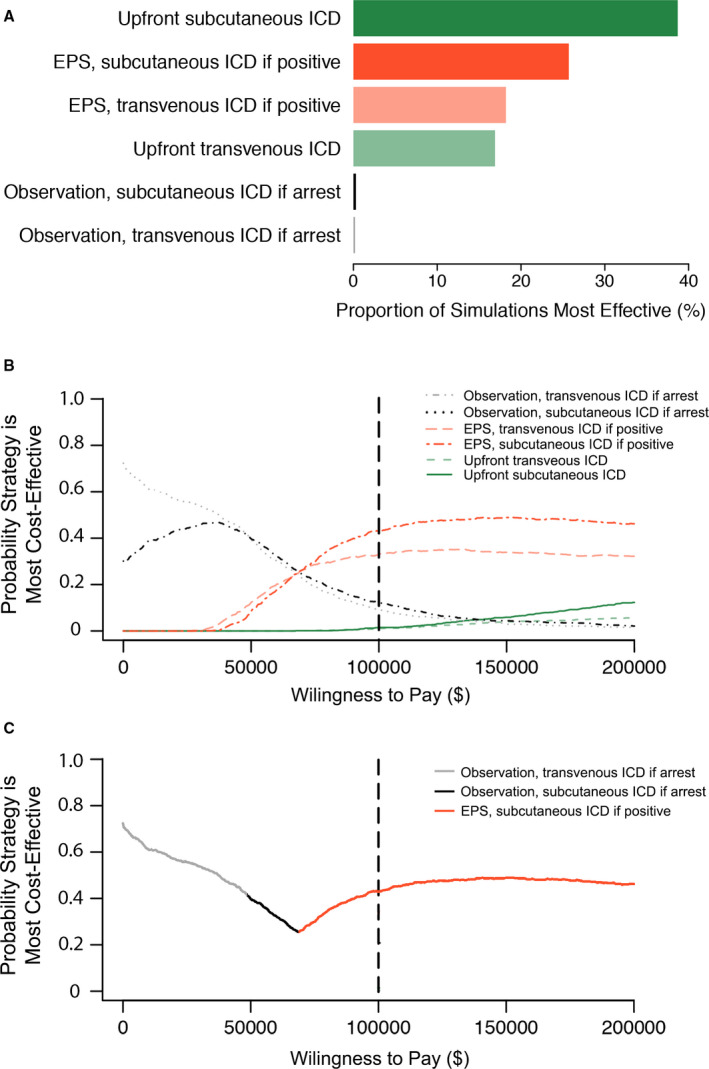
Background Optimal management of asymptomatic Brugada syndrome (BrS) with spontaneous type I electrocardiographic pattern is uncertain. Methods and Results We developed an individual-level simulation comprising 2 000 000 average-risk individuals with asymptomatic BrS and spontaneous type I electrocardiographic pattern. We compared (1) observation, (2) electrophysiologic study (EPS)-guided implantable cardioverter-defibrillator (ICD), and (3) upfront ICD, each using either subcutaneous or transvenous ICD, resulting in 6 strategies tested. The primary outcome was quality-adjusted life years (QALYs), with cardiac deaths (arrest or procedural-related) as a secondary outcome. We varied BrS diagnosis age and underlying arrest rate. We assessed cost-effectiveness at $100 000/QALY. Compared with observation, EPS-guided subcutaneous ICD resulted in 0.35 QALY gain/individual and 4130 cardiac deaths avoided/100 000 individuals, and EPS-guided transvenous ICD resulted in 0.26 QALY gain and 3390 cardiac deaths avoided. Compared with observation, upfront ICD reduced cardiac deaths by a greater margin (subcutaneous ICD, 8950; transvenous ICD, 6050), but only subcutaneous ICD improved QALYs (subcutaneous ICD, 0.25 QALY gain; transvenous ICD, 0.01 QALY loss), and complications were higher. ICD-based strategies were more effective at younger ages and higher arrest rates (eg, using subcutaneous devices, upfront ICD was the most effective strategy at ages 20-39.4 years and arrest rates >1.37%/year; EPS-guided ICD was the most effective strategy at ages 39.5-51.3 years and arrest rates 0.47%-1.37%/year, and observation was the most effective strategy at ages >51.3 years and arrest rates <0.47%/year). EPS-guided subcutaneous ICD was cost-effective ($80 508/QALY). Conclusions Device-based approaches (with or without EPS risk stratification) can be more effective than observation among selected patients with asymptomatic BrS. BrS management should be tailored to patient characteristics.
Keywords: Brugada syndrome; cost‐effectiveness; implantable defibrillator.
Conflict of interest statement
Dr Lubitz receives research support from Bristol Myers Squibb/Pfizer, Bayer AG, Boehringer Ingelheim, and Fitbit, has consulted for Bristol Myers Squibb/Pfizer and Bayer AG, and participates in a research collaboration with IBM. Dr Chhatwal received consulting fees from Novo Nordisk, Laser Europe, and Gilead Sciences, and serves as principal scientist at Value Analytics Labs. Dr Wasfy has consulted for Pfizer and Biotronik. The remaining authors have no disclosures to report.
Figures
References
-
- Sroubek J, Probst V, Mazzanti A, Delise P, Hevia JC, Ohkubo K, Zorzi A, Champagne J, Kostopoulou A, Yin X, et al. Programmed ventricular stimulation for risk stratification in the Brugada syndrome: a pooled analysis. Circulation. 2016;133:622–630. DOI: 10.1161/CIRCULATIONAHA.115.017885. - DOI - PMC - PubMed
-
- Kipp R, Hsu JC, Freeman J, Curtis J, Bao H, Hoffmayer KS. Long‐term morbidity and mortality after implantable cardioverter‐defibrillator implantation with procedural complication: a report from the National Cardiovascular Data Registry. Heart Rhythm. 2018;15:847–854. DOI: 10.1016/j.hrthm.2017.09.043. - DOI - PubMed
-
- Sears SF, Rosman L, Sasaki S, Kondo Y, Sterns LD, Schloss EJ, Kurita T, Meijer A, Raijmakers J, Gerritse B, et al. Defibrillator shocks and their effect on objective and subjective patient outcomes: results of the PainFree SST clinical trial. Heart Rhythm. 2018;15:734–740. DOI: 10.1016/j.hrthm.2017.12.026. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
