

Lower Serum Angiotensin-Converting Enzyme Level in Relation to Hyperinflammation and Impaired Antiviral Immune Response Contributes to Progression of COVID-19 Infection
- PMID: 34387835
- PMCID: PMC8361819
- DOI: 10.1007/s40121-021-00513-8
Lower Serum Angiotensin-Converting Enzyme Level in Relation to Hyperinflammation and Impaired Antiviral Immune Response Contributes to Progression of COVID-19 Infection
Abstract
Introduction: As a homologue of the angiotensin-converting enzyme (ACE), angiotensin-converting enzyme 2 (ACE2) has been identified as the main receptor for severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) invasion. We aimed to investigate the role of serum ACE in predicting the coronavirus disease 2019 (COVID-19) disease progression and the underlying mechanisms.
Methods: We retrospectively enrolled 120 patients with confirmed COVID-19 who underwent serum ACE detection on admission. The clinical characteristics and laboratory findings during hospitalization were evaluated dynamically to identify the potential risk factors for disease progression.
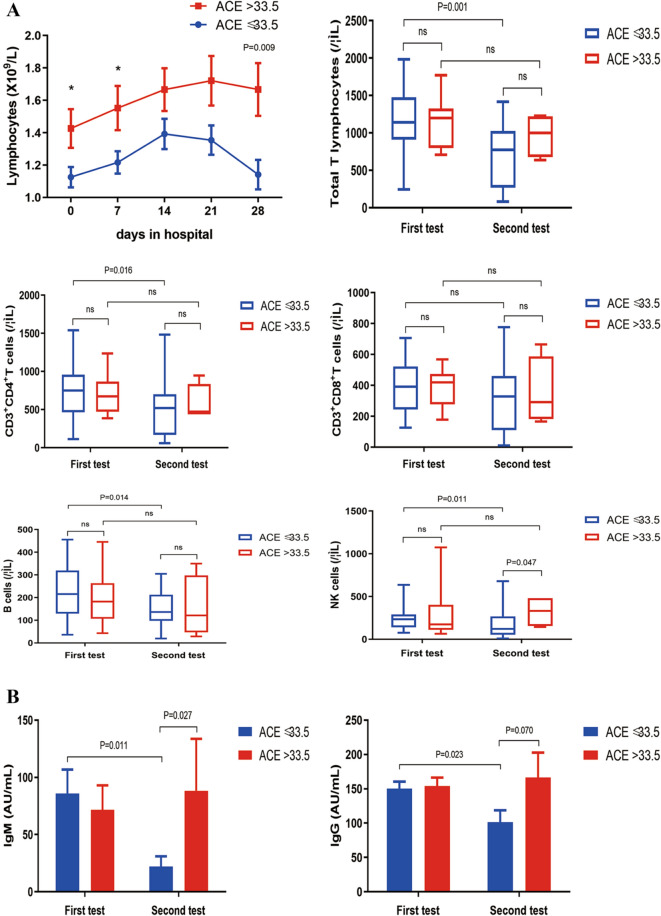
Results: ACE level was demonstrated as one of the independent risk factors. Patients with ACE level ≤ 33.5 U/L showed a higher cumulative virus RNA detection rate, elevated pro-inflammatory mediators levels, declined lymphocyte count, and decreased SARS-CoV-2-specific antibodies than those with ACE level > 33.5 U/L.
Conclusion: Lower serum ACE levels in relation to delayed virus elimination, hyperinflammatory condition, and impaired host antiviral immune responses contribute to disease progression of COVID-19.
Keywords: COVID-19; Disease progression; Immune response; Serum angiotensin-converting enzyme; Virus clearance.
© 2021. The Author(s).
Figures




References
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
